Each film-coated tablet contains 1 mg anastrozole.
Excipients/Inactive Ingredients: Lactose Monohydrate, Povidone, Sodium Starch Glycolate, Magnesium Stearate, Hypromellose, Macrogol 300, Titanium Dioxide.
Pharmacotherapeutic group: Enzyme inhibitors. ATC code: L02BG03.
Pharmacology: Pharmacodynamics: ARIMIDEX is a potent and highly selective non-steroidal aromatase inhibitor. In post-menopausal women, oestradiol is produced primarily from the conversion of androstenedione to oestrone through the aromatase enzyme complex in peripheral tissues. Oestrone is subsequently converted to oestradiol. Reducing circulating oestradiol levels has been shown to produce a beneficial effect in women with breast cancer.
In post-menopausal women, ARIMIDEX at a daily dose of 1 mg produced oestradiol suppression of greater than 80% using a highly sensitive assay.
ARIMIDEX does not possess any progestogenic, androgenic or oestrogenic activity.
Daily doses of ARIMIDEX up to 10 mg do not have any effect on cortisol or aldosterone secretion, measured before or after standard ACTH challenge testing. Corticoid supplements are therefore not needed.
Primary adjuvant treatment of early breast cancer: In a large phase III study conducted in 9366 postmenopausal women with operable breast cancer treated for 5 years, ARIMIDEX was shown to be statistically superior to tamoxifen in disease free survival. A greater magnitude of benefit was observed for disease free survival in favour of ARIMIDEX versus tamoxifen for the prospectively defined hormone receptor positive population.
ARIMIDEX was statistically superior to tamoxifen in time to recurrence. The difference was of greater magnitude than in disease free survival for both the Intention to Treat (ITT) population and hormone receptor positive population.
ARIMIDEX was statistically superior to tamoxifen in terms of time to distant recurrence. There was also a numerical trend in favour of ARIMIDEX for distant disease free survival.
The incidence of contralateral breast cancer was statistically reduced for ARIMIDEX compared to tamoxifen.
The overall survival benefit of tamoxifen was maintained with ARIMIDEX. The additional analysis of time to death following recurrence showed a numerical trend in favour of ARIMIDEX compared to tamoxifen.
Overall, ARIMIDEX was well tolerated. The following adverse events were reported regardless of causality. Patients receiving ARIMIDEX had a decrease in hot flushes, vaginal bleeding, vaginal discharge, endometrial cancer, venous thromboembolic events and ischemic cerebrovascular events compared with patients receiving tamoxifen. Patients receiving ARIMIDEX had an increase in joint disorders (including arthritis, arthrosis and arthralgia) and fractures compared with patients receiving tamoxifen. A fracture rate of 22 per 1000 patient years was observed on ARIMIDEX and 15 per 1000 patient years with the tamoxifen group with a median follow up of 68 months. The fracture rate for ARIMIDEX falls within the broad range of the fracture rates reported in an age matched postmenopausal population.
The combination of ARIMIDEX and tamoxifen did not demonstrate any efficacy benefits in comparison with tamoxifen in all patients as well as in the hormone receptor positive population. This treatment arm was discontinued from the study.
Adjuvant treatment of early breast cancer for patients being treated with adjuvant tamoxifen: In a phase III trial (ABCSG 8) conducted in 2579 postmenopausal women with hormone receptor positive early breast cancer being treated with adjuvant tamoxifen, patients had a superior disease-free survival when switched to ARIMIDEX compared with those continuing on tamoxifen.
Time to any recurrence, time to local or distant recurrence and time to distant recurrence confirmed a statistical advantage for ARIMIDEX, consistent with the results of disease free survival. The incidence of contralateral breast cancer was very low in the two treatment arms, with a numerical advantage for ARIMIDEX. Overall survival was similar for the two treatment groups.
Two further similar trials (GABG/ARNO 95 and ITA) with ARIMIDEX, as well as a combined analysis of ABCSG 8 and GABG/ARNO 95, supported these results.
The ARIMIDEX safety profile in these 3 studies was consistent with the known safety profile established in post-menopausal women with hormone-receptor positive early breast cancer.
Pharmacokinetics: Absorption of anastrozole is rapid and maximum plasma concentrations typically occur within two hours of dosing (under fasted conditions). Anastrozole is eliminated slowly with a plasma elimination half-life of 40 to 50 hours. Food slightly decreases the rate but not the extent of absorption. The small change in the rate of absorption is not expected to result in a clinically significant effect on steady-state plasma concentrations during once daily dosing of ARIMIDEX tablets. Approximately 90 to 95% of plasma anastrozole steady-state concentrations are attained after 7 daily doses. There is no evidence of time or dose-dependency of anastrozole pharmacokinetic parameters. Anastrozole pharmacokinetics is independent of age in post-menopausal women. Anastrozole is only 40% bound to plasma proteins.
Anastrozole is extensively metabolized by post-menopausal women with less than 10% of the dose excreted in the urine unchanged within 72 hours of dosing, and the remainder (about 60% of the dose) is excreted in the urine as metabolites. Metabolism of anastrozole occurs by N-dealkylation, hydroxylation and glucuronidation. The metabolites are excreted primarily via the urine. Triazole, the major metabolite in plasma, does not inhibit aromatase.
The apparent oral clearance of anastrozole in volunteers with stable hepatic cirrhosis or renal impairment was in the range observed in healthy volunteers.
Toxicology: Preclinical safety data: Acute toxicity: In acute toxicity studies in rodents the median lethal dose of anastrozole was greater than 100 mg/kg/day by the oral route and greater than 50 mg/kg/day by the intraperitoneal route. In an oral acute toxicity study in the dog the median lethal dose was greater than 45 mg/kg/day.
Chronic toxicity: Multiple dose toxicity studies utilised rats and dogs. No no-effect levels were established for anastrozole in the toxicity studies, but those effects that were observed at the low dose (1 mg/kg/day) and mid doses (dog 3 mg/kg/day; rat 5 mg/kg/day) were related to either the pharmacological or enzyme inducing properties of anastrozole, and were unaccompanied by significant toxic or degenerative changes.
Mutagenicity: Genetic toxicology studies with anastrozole show that it is not a mutagen or a clastogen.
Reproductive toxicology: Oral administration of anastrozole to pregnant rats and rabbits caused no teratogenic effects at doses up to 1.0 and 0.2 mg/kg/day, respectively. Those effects that were seen (placental enlargement in rats and pregnancy failure in rabbits) were related to the pharmacology of the compound.
Oral administration of anastrozole to female rats produced a high incidence of infertility at 1 mg/kg/day and increased pre-implantation loss at 0.02 mg/kg/day. These effects were related to the pharmacology of the compound and were completely reversed after a 5-week compound withdrawal period.
The survival of litters born to rats given anastrozole at 0.02 mg/kg/day and above (from day 17 of pregnancy to day 22 post-partum) was compromised. These effects were related to the pharmacological effects of the compound on parturition. There were no adverse effects on behaviour or reproductive performance of the first generation offspring attributable to maternal treatment with anastrozole.
Carcinogenicity: A two-year rat oncogenicity study resulted in an increase in incidence of hepatic neoplasms and uterine stromal polyps in females and thyroid adenomas in males at the high dose (25 mg/kg/day) only. These changes occurred at a dose, which represents 100-fold greater exposure than occurs at human therapeutic doses, and are considered not to be clinically relevant to the treatment of patients with anastrozole.
A two-year mouse oncogenicity study resulted in the induction of benign ovarian tumours and a disturbance in the incidence of lymphoreticular neoplasms (fewer histiocytic sarcomas in females and more deaths as a result of lymphomas). These changes are considered to be mouse-specific effects of aromatase inhibition and not clinically relevant to the treatment of patients with anastrozole.
Treatment of advanced breast cancer in post-menopausal women with oestrogen receptor positive and or progesterone receptor positive.
Adjuvant treatment of post-menopausal women with hormone receptor positive early invasive breast cancer.
Adjuvant treatment of early breast cancer in hormone receptor positive post-menopausal women, who have received 2 to 3 years of adjuvant tamoxifen.
Adults including elderly: One 1 mg tablet to be taken orally once a day. For patients with advanced breast cancer, ARIMIDEX should be continued until tumour progression.
Children: The use of ARIMIDEX is not recommended in children, as efficacy has not been established.
Renal impairment: No dose change is recommended in patients with mild or moderate renal impairment.
Hepatic impairment: No dose change is recommended in patients with mild hepatic disease.
There is limited clinical experience of overdose. In animal studies, anastrozole demonstrated low acute toxicity. Clinical trials have been conducted with various dosages of ARIMIDEX, up to 60 mg in a single dose given to healthy male volunteers and up to 10 mg daily given to post-menopausal women with advanced breast cancer; these dosages were well tolerated. A single dose of ARIMIDEX that results in life-threatening symptoms has not been established.
There is no specific antidote to overdosage and treatment must be symptomatic. In the management of an overdose, consideration should be given to the possibility that multiple agents may have been taken. Vomiting may be induced if the patient is alert. Dialysis may be helpful because ARIMIDEX is not highly protein bound. General supportive care, including frequent monitoring of vital signs and close observation of the patient, is indicated.
ARIMIDEX is contraindicated in: pre-menopausal women; pregnant or lactating women; patients with severe renal impairment (creatinine clearance less than 20 ml/min); patients with moderate or severe hepatic disease; patients with known hypersensitivity to anastrozole or to any of the excipients as referenced under Description.
Oestrogen-containing therapies should not be co-administered with ARIMIDEX as they would negate its pharmacological action.
Concurrent tamoxifen therapy (see Interactions).
ARIMIDEX is not recommended for use in children, as safety and efficacy have not been established in this group of patients.
ARIMIDEX should not be used in premenopausal women (see Contraindications). The menopause should be defined biochemically (luteinizing-hormone [LH], follicle stimulating hormone [FSH] and/or estradiol levels) in any patient where there is doubt about hormonal status. There are no data available for the use of anastrozole with LHRH analogues. This combination should not be used outside clinical trials.
There are no data to support the safe use of ARIMIDEX in patients with moderate or severe hepatic impairment, or patients with severe impairment of renal function (creatinine clearance less than 20 ml/min).
As ARIMIDEX lowers circulating oestrogen levels it may cause a reduction in bone mineral density with a possible consequent increased risk of fractures. This possible increased risk should be managed according to treatment guidelines for managing bone health in post-menopausal women.
Women with osteoporosis or at risk of osteoporosis should have their bone mineral density formally assessed by bone densitometry at the commencement of treatment and at regular intervals thereafter. Treatment or prophylaxis for osteoporosis should be initiated as appropriate and carefully monitored.
This product contains lactose. Patients with rare hereditary problems of galactose intolerance, the Lapp lactase deficiency or glucose-galactose malabsorption should not take this medicine.
Effects on ability to drive and operate machinery: ARIMIDEX is unlikely to impair the ability of patients to drive and operate machinery.
However, asthenia and somnolence have been reported with the use of ARIMIDEX and caution should be observed when driving or operating machinery while such symptoms persist.
ARIMIDEX is contraindicated in pregnant or lactating women.
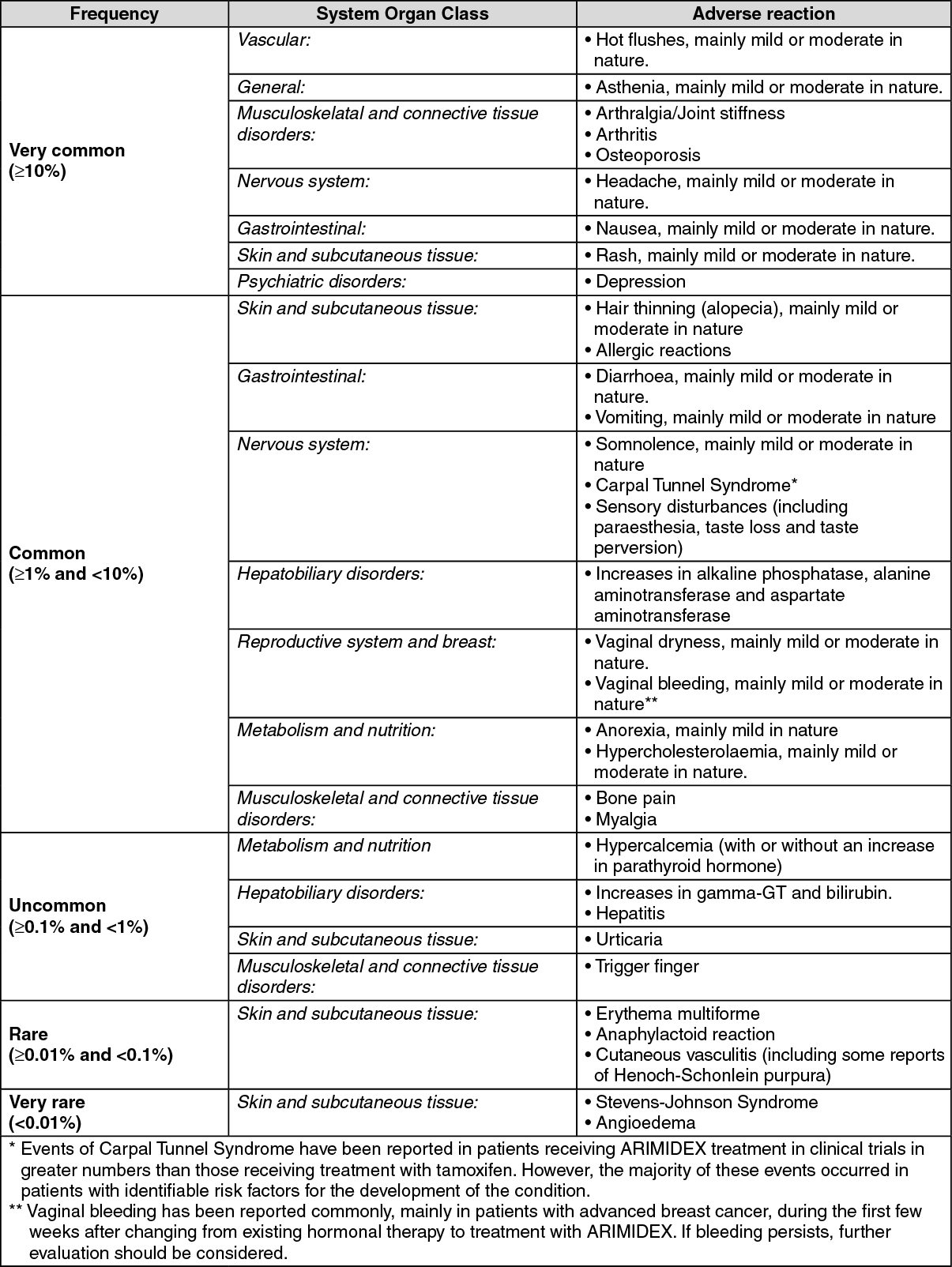
Unless specified, the following frequency categories were calculated from the number of adverse events reported in a large phase III study conducted in 9366 post-menopausal women with operable breast cancer treated for 5 years and unless specified, no account was taken of the frequency within the comparative treatment group or whether the investigator considered it to be related to study medication. (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
As ARIMIDEX lowers circulating oestrogen levels, it may cause a reduction in bone mineral density placing some patients at a higher risk of fracture (see Precautions).
In a large phase III study conducted in 9366 postmenopausal women with operable breast cancer treated for 5 years, ischaemic cardiovascular events were reported more frequently in patients treated with ARIMIDEX compared to those treated with tamoxifen, although the difference was not statistically significant. The observed difference was mainly due to more reports of angina pectoris and was associated with a sub-group of patients with pre-existing ischaemic heart disease.
Antipyrine and cimetidine clinical interaction studies indicate that the co-administration of ARIMIDEX with other drugs is unlikely to result in clinically significant drug interactions mediated by cytochrome P450.
A review of the clinical trial safety database did not reveal evidence of clinically significant interaction in patients treated with ARIMIDEX who also received other commonly prescribed drugs.
Tamoxifen and/or other therapies containing oestrogen should not be co-administered with ARIMIDEX, as they may diminish its pharmacological action (see Contraindications).
Incompatibilities: Not applicable.
Do not store above 30°C.
Shelf-life: 5 years.
L02BG03 - anastrozole ; Belongs to the class of enzyme inhibitors. Used in treatment of neoplastic diseases.
Arimidex FC tab 1 mg
2 × 14's (Rp2,903,857/boks)


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out