


 Sign Out
Sign Out
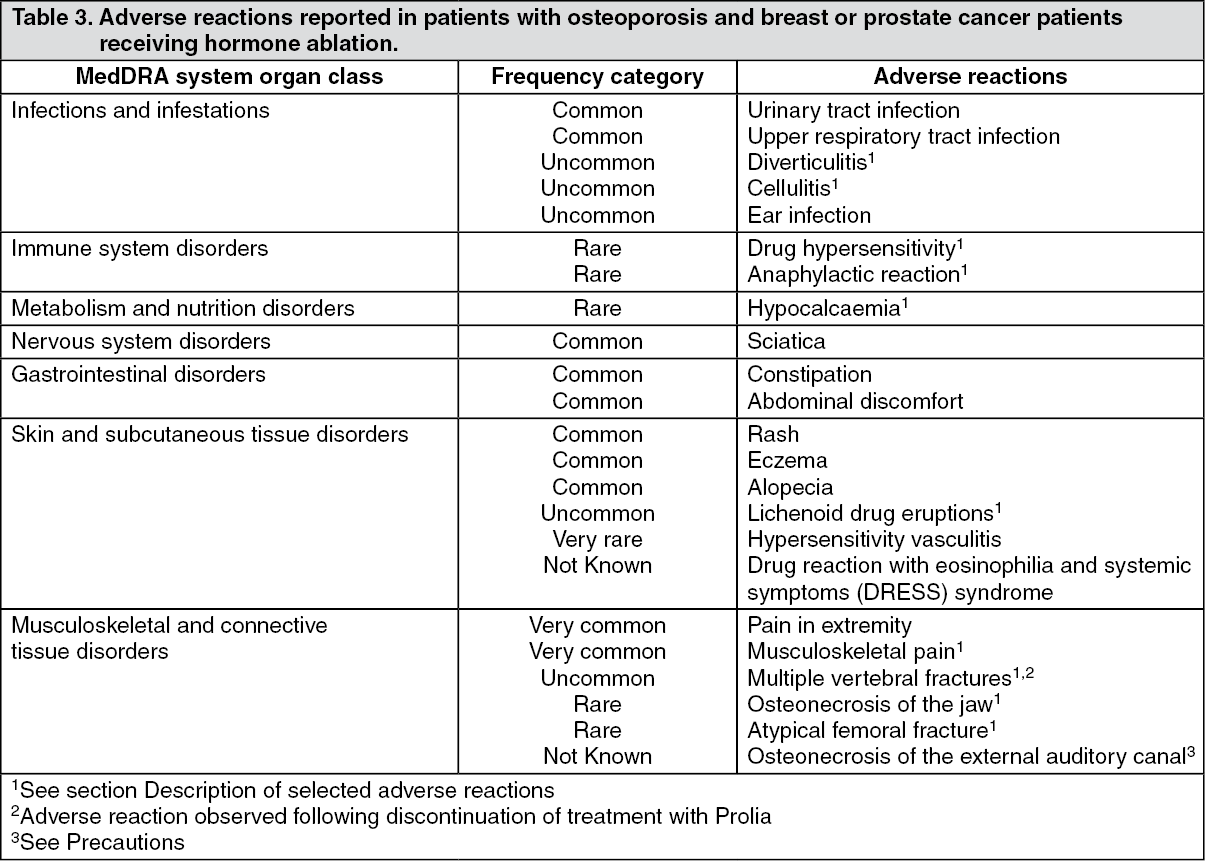
Tabulated list of adverse reactions: The data in Table 3 as follows describe adverse reactions reported from Phase II and III clinical trials in patients with osteoporosis and breast or prostate cancer patients receiving hormone ablation; and/or spontaneous reporting.
The following convention has been used for the classification of the adverse reactions (see table 1): very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1,000 to < 1/100), rare (≥ 1/10,000 to < 1/1,000), very rare (< 1/10,000) and not known (cannot be estimated from the available data). Within each frequency grouping and system organ class, adverse reactions are presented in order of decreasing seriousness. (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn a pooled analysis of data from all phase II and phase III placebo controlled studies, Influenza-like illness was reported with a crude incidence rate of 1.2% for denosumab and 0.7 % for placebo. Although this imbalance was identified via a pooled analysis, it was not identified via a stratified analysis.
Description of selected adverse reactions: Hypocalcaemia: In two phase III placebo-controlled clinical trials in postmenopausal women with osteoporosis, approximately 0.05% (2 out of 4,050) of patients had declines of serum calcium levels (less than 1.88 mmol/l) following Prolia administration. Declines of serum calcium levels (less than 1.88 mmol/l) were not reported in either the two phase III placebo-controlled clinical trials in patients receiving hormone ablation or the phase III placebo-controlled clinical trial in men with osteoporosis.
In the post-marketing setting, rare cases of severe symptomatic hypocalcaemia have been reported predominantly in patients at increased risk of hypocalcaemia receiving Prolia, with most cases occurring in the first weeks of initiating therapy. Examples of the clinical manifestations of severe symptomatic hypocalcaemia have included QT interval prolongation, tetany, seizures and altered mental status (see Precautions). Symptoms of hypocalcaemia in denosumab clinical studies included paraesthesias or muscle stiffness, twitching, spasms and muscle cramps.
Skin infections: In phase III placebo-controlled clinical trials, the overall incidence of skin infections was similar in the placebo and the Prolia groups: in postmenopausal women with osteoporosis (placebo [1.2%, 50 out of 4,041] versus Prolia [1.5%, 59 out of 4,050]); in men with osteoporosis (placebo [0.8%, 1 out of 120] versus Prolia [0%, 0 out of 120]); in breast or prostate cancer patients receiving hormone ablation (placebo [1.7%, 14 out of 845] versus Prolia [1.4%, 12 out of 860]). Skin infections leading to hospitalisation were reported in 0.1% (3 out of 4,041) of postmenopausal women with osteoporosis receiving placebo versus 0.4% (16 out of 4,050) of women receiving Prolia. These cases were predominantly cellulitis. Skin infections reported as serious adverse reactions were similar in the placebo (0.6%, 5 out of 845) and the Prolia (0.6%, 5 out of 860) groups in the breast and prostate cancer studies.
Osteonecrosis of the jaw: ONJ has been reported rarely, in 16 patients, in clinical trials in osteoporosis and in breast or prostate cancer patients receiving hormone ablation including a total of 23,148 patients (see Precautions). Thirteen of these ONJ cases occurred in postmenopausal women with osteoporosis during the phase III clinical trial extension following treatment with Prolia for up to 10 years. Incidence of ONJ was 0.04% at 3 years, 0.06% at 5 years and 0.44% at 10 years of Prolia treatment. The risk of ONJ increased with duration of exposure to Prolia.
Atypical fractures of the femur: In the osteoporosis clinical trial program, atypical femoral fractures were reported rarely in patients treated with Prolia (see Precautions).
Diverticulitis: In a single phase III placebo-controlled clinical trial in patients with prostate cancer receiving ADT an imbalance in diverticulitis adverse events was observed (1.2% denosumab, 0% placebo). The incidence of diverticulitis was comparable between treatment groups in postmenopausal women or men with osteoporosis and in women undergoing aromatase inhibitor therapy for non-metastatic breast cancer.
Drug-related hypersensitivity reactions: In the post-marketing setting, rare events of drug-related hypersensitivity, including rash, urticaria, facial swelling, erythema, and anaphylactic reactions have been reported in patients receiving Prolia.
Musculoskeletal pain: Musculoskeletal pain, including severe cases, has been reported in patients receiving Prolia in the post-marketing setting. In clinical trials, musculoskeletal pain was very common in both denosumab and placebo groups. Musculoskeletal pain leading to discontinuation of study treatment was uncommon.
Multiple Vertebral Fractures following discontinuation of Prolia treatment: In the osteoporosis clinical trial program, MVF were reported uncommonly in patients following discontinuation of treatment with Prolia, particularly in those with a history of vertebral fracture.
Lichenoid drug eruptions: Lichenoid drug eruptions (e.g. lichen planus-like reactions), have been reported in patients in the post-marketing setting.
Other special populations: Paediatric population: Prolia should not be used in paediatric patients (age < 18). Serious hypercalcaemia has been reported. Some clinical trial cases were complicated by acute renal injury.
Renal impairment: In clinical studies, patients with severe renal impairment (creatinine clearance < 30 mL/min) or receiving dialysis were at greater risk of developing hypocalcaemia in the absence of calcium supplementation. Adequate intake of calcium and vitamin D is important in patients with severe renal impairment or receiving dialysis (see Precautions).
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit-risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions as per local regulations.
View ADR Monitoring Form