


 Sign Out
Sign Out
 Click on icon to see table/diagram/image
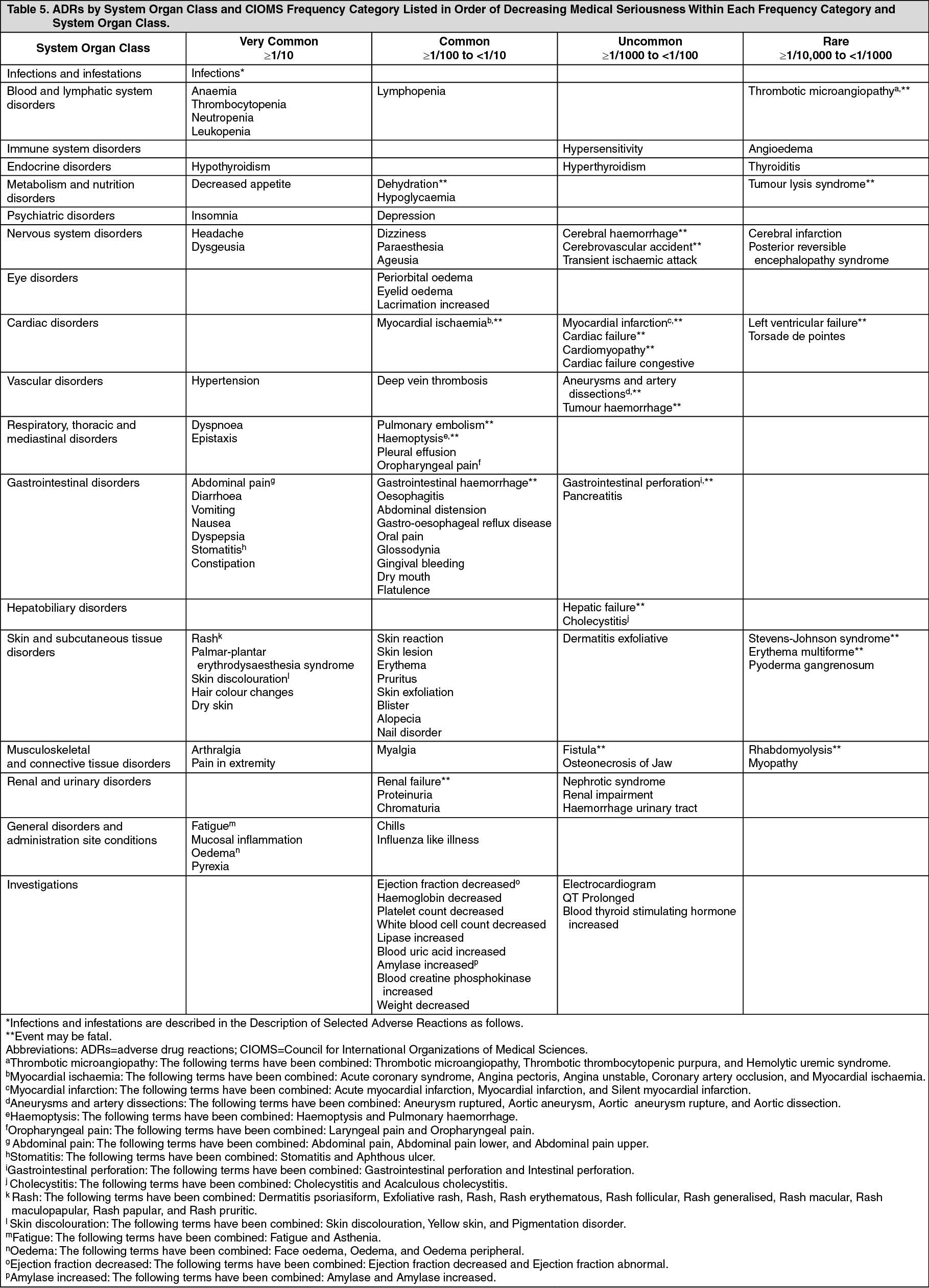
Click on icon to see table/diagram/imageADR frequencies presented previously represent the frequencies of the events that occurred in sunitinib-treated subjects regardless of causality assessment.
The most important serious adverse reactions associated with sunitinib treatment of patients with solid tumors‡⁎ were pulmonary embolism, thrombocytopenia, tumor hemorrhage, febrile neutropenia, and hypertension (see Precautions).
The most common ADRs of any grade included: fatigue; gastrointestinal disorders, such as diarrhea, nausea, stomatitis, dyspepsia, and vomiting; skin discoloration; rash; palmar plantar erythrodysesthesia; dry skin; hair color changes; mucosal inflammation; asthenia; dysgeusia; anorexia and hypertension. Fatigue, hypertension and neutropenia were the most common ADRs of Grade 3 maximum severity, and increased lipase was the most frequently occurring ADRs of Grade 4 maximum severity in subjects with solid tumors.
Epistaxis, was the most frequent hemorrhagic ADR, having been reported for approximately half of the subjects with solid tumors* who experienced hemorrhagic events (see Precautions).
In clinical studies of sunitinib, seizures have been observed in subjects with radiological evidence of brain metastases. In addition, there have been reports (<1%), some fatal, of subjects presenting with seizures and radiological evidence of RPLS (see Precautions).
Description of Selected Adverse Reactions: Infections and Infestations: Cases of serious infection (with or without neutropenia), in some cases with fatal outcome, have been reported. The infections observed with sunitinib treatment are infections typically seen in cancer patients, e.g., respiratory infections (e.g., pneumonia, bronchitis), urinary tract infections, skin infections (e.g., cellulitis), sepsis/septic shock, and abscess (e.g., oral, genital, anorectal, skin, limb, visceral). Infections may be bacterial, viral, or fungal. Rare cases of necrotizing fasciitis, including of the perineum, sometimes fatal, have been reported.
Blood and Lymphatic System Disorders: Rare cases of thrombotic microangiopathy, in some cases with fatal outcome, have been reported. Temporary suspension of sunitinib is recommended; following resolution, treatment may be resumed at the discretion of the treating physician.
Vascular Disorders: Arterial Thromboembolic Events (ATE): Cases of arterial thromboembolic events (ATE), sometimes fatal, have been reported in patients treated with sunitinib. The most frequent events included cerebrovascular accident, transient ischaemic attack and cerebral infarction. Risk factors associated with ATE, in addition to the underlying malignant disease and age ≥65 years, included hypertension, diabetes mellitus, and prior thromboembolic disease.
*From initial clinical trials including primarily patients with GIST and cytokine-refractory advanced RCC.
Venous Thromboembolic Events (VTE): In the double-blind treatment phase of GIST study, 7 patients (3%) on sunitinib and none on placebo experienced VTE; 5 of the 7 were Grade 3 deep vein thrombosis (DVT), and 2 were Grade 1 or 2. Four of these 7 GIST patients discontinued treatment following first observation of DVT. Thirteen patients (3%) receiving sunitinib for treatment-naïve advanced RCC and 4 (2%) patients in the 2 cytokine-refractory advanced RCC studies had VTE reported. Nine of these patients had pulmonary embolism: 1 was Grade 2 and 8 were Grade 4. Eight patients had DVT: 1 with Grade 1, 2 with Grade 2, 4 with Grade 3, and 1 with Grade 4. One patient with pulmonary embolism in the cytokine-refractory advanced RCC study experienced dose interruption. In treatment-naïve advanced RCC patients receiving IFN-α, 6 (2%) VTE occurred; 1 (<1%) patient experienced a Grade 3 DVT and 5 (1%) patients had pulmonary embolism, all Grade 4.
Pulmonary embolism was reported in approximately 2.2% of patients with solid tumors‡ who received sunitinib. None of these events resulted in a patient discontinuing treatment with sunitinib; however, a dose reduction or temporary delay in treatment occurred in a few cases. There were no further occurrences of pulmonary embolism in these patients after treatment was resumed.
‡ From initial clinical trials including primarily patients with GIST and cytokine-refractory advanced RCC. Musculoskeletal and Connective Tissue Disorders: Rare cases of myopathy and/or rhabdomyolysis with or without acute renal failure, in some cases with fatal outcome, have been reported. Most of these patients had pre-existing risk factors and/or were receiving concomitant medications known to be associated with these adverse reactions. Patients with signs or symptoms of muscle toxicity should be managed as per standard medical practice.
Long-term Safety in RCC: The long-term safety of sunitinib in patients with metastatic RCC was analyzed across 9 completed clinical studies conducted in the first-line, bevacizumab-refractory and cytokine-refractory treatment settings. The analysis included 5739 patients, of whom 807 (14%) were treated for ≥2 years up to 6 years. Prolonged treatment with sunitinib was not associated with new types or increased severity of treatment-related adverse events and except for hypothyroidism, toxicity was not cumulative.
View ADR Monitoring Form