Each tablet contains memantine HCl 10 mg corresponding to 8.31 mg memantine (free base). It also contains the following inactive excipients: Lactose monohydrate, microcrystalline cellulose, colloidal anhydrous silica, talc, magnesium stearate, methacrylic acid ethyl acrylate copolymer (1:1), sodium lauryl sulfate, polysorbate 80, triacetin and simethicone emulsion.
Anti-dementia.
Pharmacology: There is increasing evidence that malfunctioning of glutamatergic neurotransmission, in particular at NMDA-receptors, contributes to both expression of symptoms and disease progression in neurodegenerative dementia.
Memantine is a voltage-dependent, moderate-affinity uncompetitive NMDA-receptor antagonist. It modulates the effects of pathologically elevated tonic levels of glutamate that may lead to neuronal dysfunction.
Clinical Studies: A clinical trial in a population of patients suffering from moderate to severe Alzheimer's disease (MMSE total scores at baseline of 3-14) showed beneficial effects of memantine treatment in comparison to placebo over a treatment period of 6 months.
In this multicenter, double-blind, randomized, placebo-controlled study, a total of 252 outpatients (33% male, 67% female, mean age 76 years) were included. The dosing was 10 mg memantine twice a day. Primary outcome parameters included assessment of the global domain [using the Clinicians Interview-Based Impression of Change (CIBIC-Plus)] and the functional domain [using the Activities of Daily Living Inventory (ADCS-ADLsev)]. Cognition was assessed as a secondary endpoint with the Severe Impairment Battery (SIB). The results in these domains favoured memantine over placebo (Observed Cases Analysis for CIBIC-Plus: p=0.025; ADCS-ADLsev: p=0.003; SIB: p=0.002).
After 6 months, the rate of individual responders (response prospectively defined as stabilization or improvement in 2 independent domains) was 29% for the memantine group versus 10% for placebo (p=0.0004). With a triple criterion (response defined as stabilization or improvement in all 3 domains: Cognition, functional and global domain), there were 11% responders for memantine versus 6% for placebo (p=0.17).
Pharmacokinetics: Absorption: Memantine has an absolute bioavailability of approximately 100%. Tmax is between 3 and 8 hrs. There is no indication that food influences the absorption of memantine.
Linearity: Studies in volunteers have demonstrated linear pharmacokinetics in the dose range of 10-40 mg.
Distribution: Daily doses of 20 mg lead to steady-state plasma concentrations of memantine ranging from 70-150 ng/mL (0.5-1 micromole) with large interindividual variations. When daily doses of 5-30 mg were administered, a mean CSF/serum ratio of 0.52 was calculated. The volume of distribution is around 10 L/kg. About 45% of memantine is bound to plasma proteins.
Biotransformation: In man, about 80% of the circulating memantine-related material is present as the parent compound. Main human metabolites are N-3,5-dimethyl-gludantan, the isomeric mixture of 4- and 6-hydroxy-memantine, and 1-nitroso-3,5-dimethyl-adamantane. None of these metabolites exhibit NMDA-antagonistic activity. No cytochrome P-450 catalyzed metabolism has been detected in vitro.
In a study using orally administered 14C-memantine, a mean of 84% of the dose was recovered within 20 days, >99% being excreted renally.
Elimination: Memantine is eliminated in a monoexponential manner with a terminal t½ of 60-100 hrs. In volunteers with normal kidney function, total clearance (Cltot) amounts to 170 mL/min/1.73 m2 and part of total renal clearance is achieved by tubular secretion.
Renal handling also involves tubular reabsorption, probably mediated by cation transport proteins. The renal elimination rate of memantine under alkaline urine conditions may be reduced by a factor of 7-9 (see Precautions). Alkalization of urine may result from drastic changes in diet eg, from a carnivore to a vegetarian diet, or from the massive ingestion of alkalizing gastric buffers.
Specific Patient Population: In elderly volunteers with normal and reduced renal function (CrCl of 50-100 mL/min/1.73 m2), a significant correlation was observed between CrCl and total renal clearance of memantine (see Dosage & Administration).
The effect of liver disease on the pharmacokinetics of memantine has not been studied. As memantine is metabolized to a minor extent only, and into metabolites with no NMDA-antagonistic activity, clinically relevant changes in the pharmacokinetics are not expected in mild to moderate liver impairment.
Pharmacokinetic/Pharmacodynamic Relationship: At a dose of memantine of 20 mg/day the cerebrospinal fluid (CSF) levels match the ki-value (ki=inhibition constant) of memantine, which is 0.5 micromole in human frontal cortex.
Toxicology: Preclinical Safety Data: In short-term studies in rats, memantine like other NMDA-antagonists has induced neuronal vacuolisation and necrosis (Olney lesions) only after doses leading to very high peak serum concentrations. Ataxia and other preclinical signs have preceded the vacuolisation and necrosis. As the effects have neither been observed in long-term studies in rodents nor in non-rodents, the clinical relevance of these findings is unknown.
Ocular changes were inconsistently observed in repeated dose toxicity studies in rodents and dogs, but not in monkeys. Specific ophthalmoscopic examinations in clinical studies with memantine did not disclose any ocular changes.
Phospholipidosis in pulmonary macrophages due to accumulation of memantine in lysosomes was observed in rodents. This effect is known from other drugs with cationic amphiphilic properties. There is a possible relationship between this accumulation and the vacuolisation observed in lungs. This effect was only observed at high doses in rodents. The clinical relevance of these findings is unknown.
No genotoxicity has been observed following testing of memantine in standard assays. There was no evidence of any carcinogenicity in life-long studies in mice and rats. Memantine was not teratogenic in rats and rabbits, even at maternally toxic doses, and no adverse effects of memantine were noted on fertility. In rats, foetal growth reduction was noted at exposure levels which are identical or slightly higher than at human exposure.
Treatment of patients with moderate to severe Alzheimer's disease.
Treatment should be initiated and supervised by a physician experienced in the diagnosis and treatment of Alzheimer's dementia. Therapy should only be started if a caregiver is available who will regularly monitor drug intake by the patient. Diagnosis should be made according to current guidelines.
The tablets can be taken with or without food.
Adults: Maximum Daily Dose: 20 mg/day. In order to reduce the risk of side effects, the maintenance dose is achieved by upward titration 5 mg/week over the first 3 weeks as follows: Treatment should be started with 5 mg daily (½ tab in the morning) during the 1st week. In the 2nd week, 10 mg/day (½ tab twice a day) and in the 3rd week 15 mg/day is recommended (1 tab in the morning and ½ tab in the afternoon). From the 4th week on, treatment can be continued with the recommended maintenance dose of 20 mg/day (1 tab twice a day).
Elderly >65 years: Recommended Dose: 20 mg/day (10 mg twice a day) as previously described.
Children and Adolescents <18 years: The safety and efficacy of memantine in children and adolescents have not been established.
Renal Impairment: In patients with normal to mildly impaired renal function (serum creatinine levels of up to 130 micromole/L) no dose reduction is needed. In patients with moderate renal impairment (CrCl 40-60 mL/min/1.73 m2) daily dose should be reduced to 10 mg/day. No data are available for patients with severely reduced kidney function (see Precautions and Pharmacokinetics under Actions).
Hepatic Impairment: There are no data on the use of memantine in patients with hepatic impairment (see Pharmacokinetics under Actions).
In 1 case of suicidal overdosage the patient survived the oral intake of up to 400 mg memantine with effects on the central nervous system (eg, restlessness, psychosis, visual hallucinations, proconvulsiveness, somnolence, stupor and unconsciousness) which resolved without permanent sequelae.
Treatment of overdosage should be symptomatic.
Hypersensitivity to memantine or to any of the excipients of Abixa.
As no data are available for patients with severe renal impairment (CrCl <9 mL/min/1.73 m2) therapy is not recommended (see Dosage & Administration).
Based on pharmacological considerations and single case reports, caution is recommended with patients suffering from epilepsy.
Concomitant use of N-methyl-D-aspartate (NMDA)-antagonists eg, amantadine, ketamine or dextromethorphan should be avoided. These compounds act at the same receptor system as memantine, and therefore, adverse drug reactions (mainly CNS-related) may be more frequent or more pronounced (see Interactions).
Some factors that may raise urine pH (see Pharmacokinetics: Elimination under Actions) may necessitate careful monitoring of the patient. These factors include drastic changes in diet eg, from a carnivore to a vegetarian diet, or a massive ingestion of alkalizing gastric buffers. Also, urine pH may be elevated by states of renal tubulary acidosis (RTA) or severe infections of the urinary tract with Proteus bacteria.
In most clinical trials, patients with recent myocardial infarction, uncompensated congestive heart failure (NYHA III-IV) or uncontrolled hypertension were excluded. As a consequence, only limited data are available and patients with these conditions should be closely supervised.
Effects on the Ability to Drive or Operate Machinery: Moderate to severe Alzheimer's disease usually causes impairment of driving performance and compromises the ability to use machinery. Furthermore, memantine may change reactivity such that outpatients should be warned to take special care when driving a vehicle or operating machinery.
Use in pregnancy & lactation: For memantine, no clinical data on exposed pregnancies are available. Animal studies indicate a potential for reducing intrauterine growth at exposure levels which are identical or slightly higher than at human exposure (see Toxicology under Actions). The potential risk for humans is unknown. Memantine should not be used during pregnancy unless clearly necessary.
It is not known whether memantine is excreted in human's breast milk but, taking into consideration the lipophilicity of the substance, this probably occurs. Women taking memantine should not breastfeed.
For memantine, no clinical data on exposed pregnancies are available. Animal studies indicate a potential for reducing intrauterine growth at exposure levels which are identical or slightly higher than at human exposure (see Toxicology under Actions). The potential risk for humans is unknown. Memantine should not be used during pregnancy unless clearly necessary.
It is not known whether memantine is excreted in human's breast milk but, taking into consideration the lipophilicity of the substance, this probably occurs. Women taking memantine should not breastfeed.
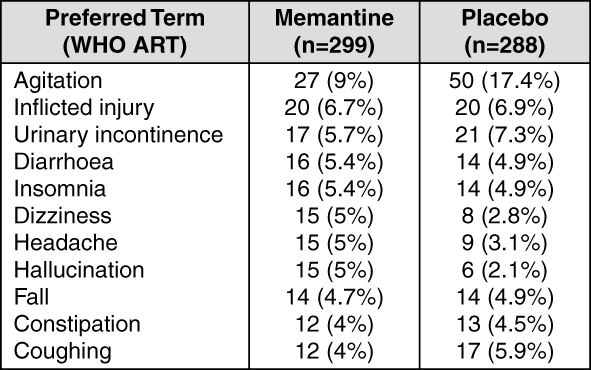
In clinical trials in moderate to severe dementia, overall incidence rates for adverse events did not differ from placebo treatment and adverse events were usually mild to moderate in severity.
The following table gives an overview of the most frequent (>4% for memantine) adverse events (irrespective of causal relationship) that were observed in the trial population of patients with moderate to severe dementia. (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Common adverse reactions (1-10% and more frequent than with placebo) for memantine and placebo patients respectively were: Hallucinations (2% vs 0.7%), confusion (1.3% vs 0.3%), dizziness (1.7% vs 1%), headache (1.7% vs 1.4%) and tiredness (1% vs 0.3%).
Uncommon adverse reactions (0.1-1% and more frequent than with placebo) were anxiety, hypertonia (increased muscle tone), vomiting, cystitis and increased libido.
Due to the pharmacological effects and the mechanism of action of memantine the following interactions may occur: The mode of action suggests that the effects of L-dopa, dopaminergic agonists and anticholinergics may be enhanced by concomitant treatment with NMDA-antagonists eg, memantine. The effects of barbiturates and neuroleptics may be reduced. Concomitant administration of memantine with the antispasmodic agents, dantrolene or baclofen, can modify their effects and a dosage adjustment may be necessary.
Concomitant use of memantine and amantadine should be avoided, owing to the risk of pharmacotoxic psychosis. Both compounds are chemically related NMDA-antagonists. The same may be true for ketamine and dextromethorphan (see Precautions). There is 1 published case report on a possible risk also for the combination of memantine and phenytoin.
Other drugs eg, cimetidine, ranitidine, procainamide, quinidine, quinine and nicotine that use the same renal cationic transport system as amantadine may also possibly interact with memantine leading to a potential risk of increased plasma levels.
There may be a possibility of slightly reduced serum level of hydrochlorothiazide (HCTZ) when memantine is co-administered with HCTZ or any combination with HCTZ.
Memantine did not inhibit CYP1A2, 2A6, 2C9, 2D6, 2E1, 3A, flavin containing monooxygenase, epoxide hydrolase and sulphation in vitro.
Incompatibilities: Not applicable.
Store at temperature not exceeding 30°C.
N06DX01 - memantine ; Belongs to the class of other anti-dementia drugs.
Abixa FC tab 10 mg
28's (P3,535.72/pack)
Abixa FC tab 20 mg
28's (P6,364.29/pack)




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out