Dermal safety studies involving induction and challenge phases produced no evidence that Imiquimod (Aldara) Cream causes photoallergenicity or contact sensitization in healthy skin; however, cumulative irritancy testing revealed the potential for Imiquimod (Aldara) Cream to cause irritation and in the clinical studies application site reactions were reported in a significant percentage of study patients. Phototoxicity testing was incomplete as wavelengths in the UVB range were not included and Aldara has peak absorption in the UVB range (320 nm) of the light spectrum.
External Genital Warts: In controlled clinical trials, the most frequently reported adverse reaction were those of local skin and application site reactions; some patients also reported systemic reactions. These reactions were usually mild to moderate in intensity; however, severe reactions were reported with 3X/week application. These reactions were more frequent and more intense with daily application than with 3 times per week application. Overall, in the 3X/week application clinical studies, 1.2% (4/327) of the patients discontinued due to local skin/application site reaction.
The incidence and severity of local skin reactions during controlled clinical trials are shown in the following table. (See Table 6.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Remote site skin reactions were also reported in female and male patients treated 3 times per week with Imiquimod (Aldara) 5% Cream. The severe remote site skin reactions reported for females were erythema (3%), ulceration (2%) and edema (1%) and for males, erosion (2%) and erythema, edema, induration and excoriation/flaking (each 1%).
Adverse events judged to be probably or possibly related to Imiquimod (Aldara) Cream reported by >5% of patients are listed in Table 7; also included are soreness, influenza-like symptoms and myalgia. (See Table 7.)
Click on icon to see table/diagram/image
Adverse events judged to be possibility or probability related to Aldara and reported by >1% of patients includes:
Application Site Disorders: Wart site reactions (burning, hypopigmentation, irritation, itching, pain, rash, sensitivity, soreness, stinging, tenderness).
Remote Site Reactions: Bleeding, burning, itching, pain, tenderness, tinea cruris.
Body as a Whole: Fatigue, fever, influenza-like symptoms.
Central and Peripheral Nervous System Disorders: Headache.
Gastrointestinal System Disorders: Diarrhea.
Musculoskeletal System Disorders: Myalgia.
Superficial Basal Cell Carcinoma: The data described in the following text reflect exposure to Aldara or vehicle in 364 patients enrolled in 2 double-blind, vehicle-controlled, 5 times per week studies. Patients applied Imiquimod (Aldara) Cream or vehicle 5X/week for 6 weeks. The incidence of adverse events reported by >1% of subjects during the 6 week treatment period is summarized in the following table. (See Table 8.)
Click on icon to see table/diagram/image
In controlled clinical studies, the most frequently reported adverse reactions were local skin and application site reactions including erythema, edema, induration, erosion, flaking/scaling, scabbing/crusting, itching and burning at the application site.
The incidence of the application site reactions reported by >1% of the subjects during the 6 weeks treatment period is summarized in the following table. (See Table 9.)
Click on icon to see table/diagram/image
Local skin reactions were collected independently of the adverse event "application site reaction" in an effort to provide a better picture of specific types of local reactions that might be seen. The prevalence and severity of local skin reactions that occurred during controlled studies are shown in the following table. (See Table 10.)
Click on icon to see table/diagram/image
The adverse reactions that most frequently resulted in clinical intervention (e.g., rest periods, withdrawal from study) were local skin and application site reactions; 10% (19/185) of patients received rest periods. The average number of doses not received per patients due to rest periods was 7 doses with a range of 2 to 22 doses; 79% of patients (15/19) resumed therapy after a rest period. Overall, in the clinical studies, 2% (4/185) of patients discontinued for local skin/application site reactions. In the sBCC studies, 17 of 1266 (1.3%) imiquimod-treated patients developed treatment site infections that required a rest period off Imiquimod (Aldara) Cream and were treated with antibiotics.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image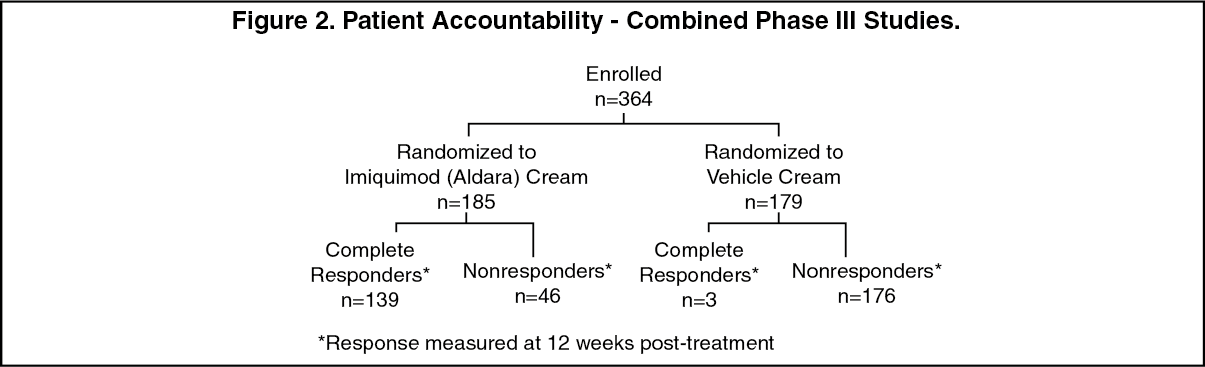 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image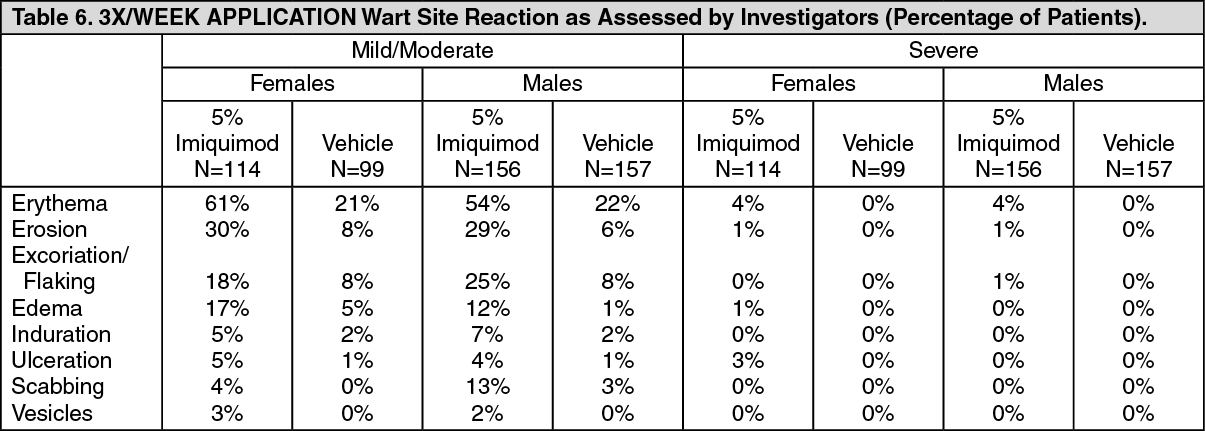 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image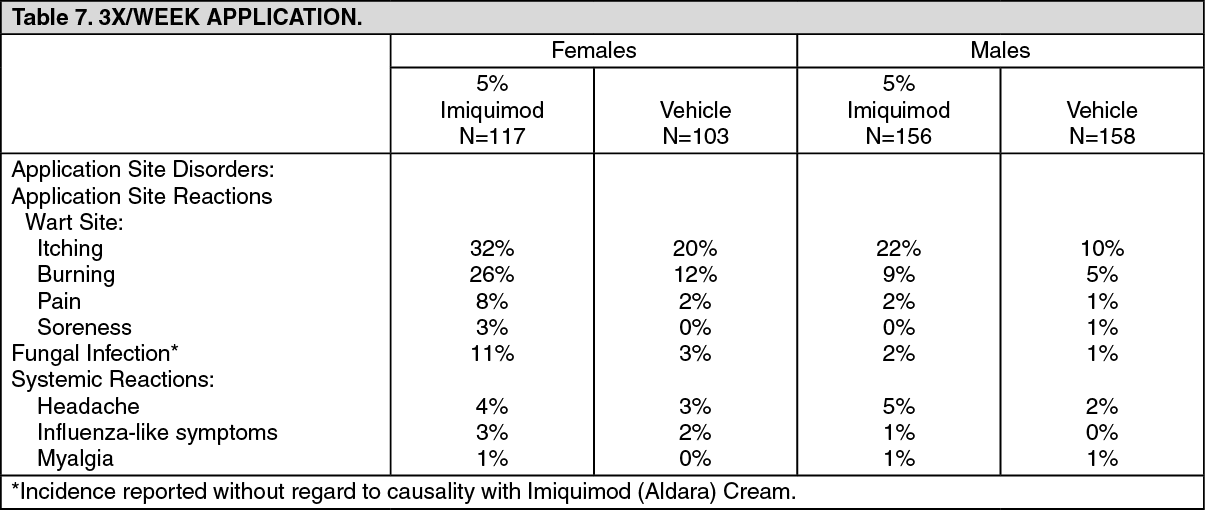 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image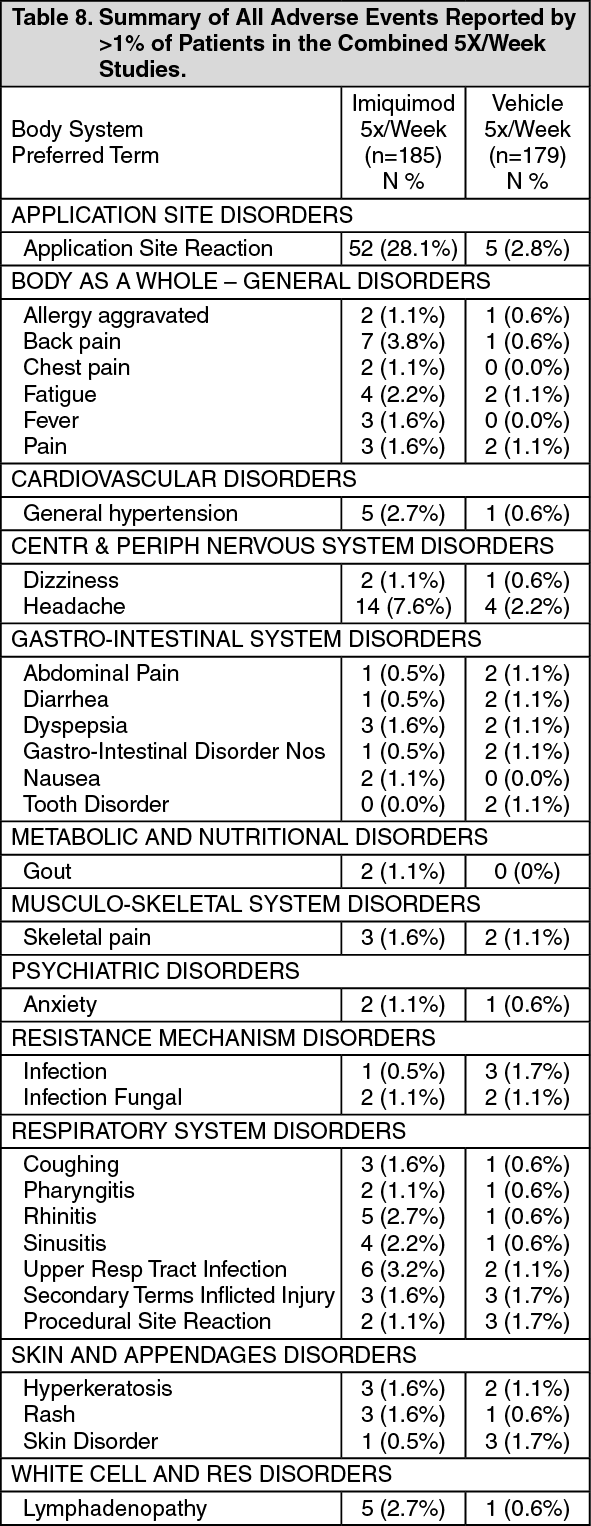 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image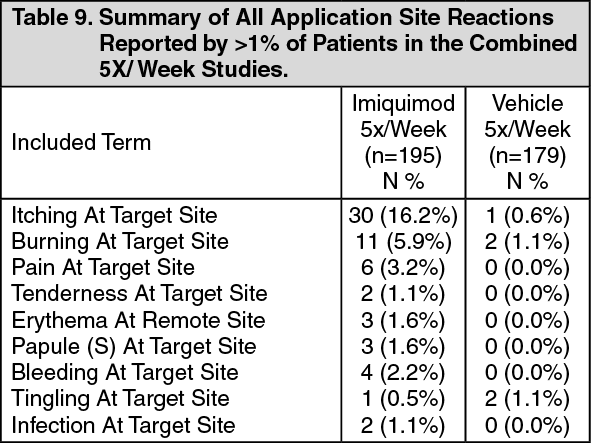 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image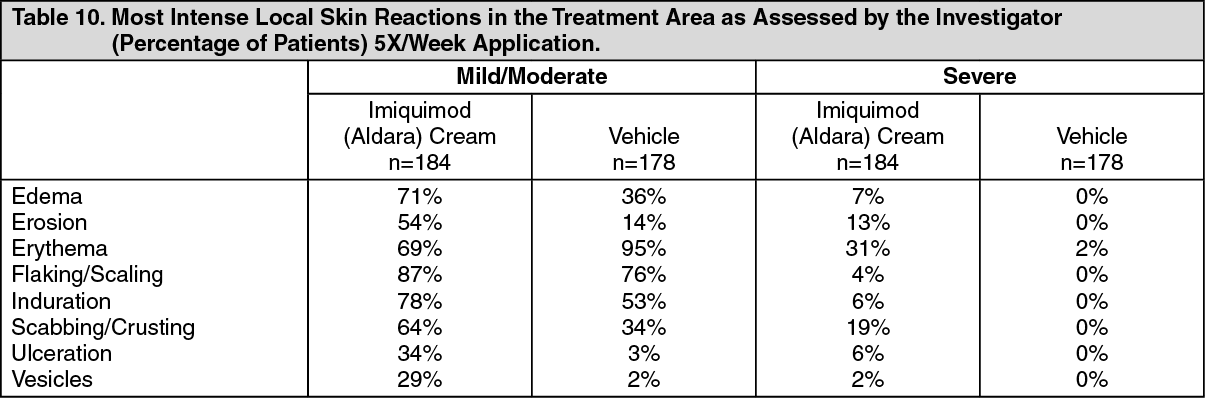 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
