


 Sign Out
Sign Out
Pharmacology: Pharmacodynamics: Exemestane is an irreversible, steroidal aromatase inhibitor, structurally related to the natural substrate androstenedione. In postmenopausal women, oestrogens are produced primarily from the conversion of androgens into oestrogens through the aromatase enzyme in peripheral tissues. Oestrogen deprivation through aromatase inhibition is an effective and selective treatment for hormone-dependent breast cancer in postmenopausal women. In postmenopausal women, exemestane p.o. significantly lowered serum oestrogen concentrations starting from a 5 mg dose, reaching maximal suppression (>90%) with a dose of 10-25 mg. In postmenopausal breast cancer patients treated with the 25 mg daily dose, whole body aromatisation was reduced by 98%.
Exemestane does not possess any progestogenic or oestrogenic activity. A slight androgenic activity, probably due to the 17-hydro derivative, has been observed mainly at high doses. In multiple daily dose trials, exemestane had no detectable effects on adrenal biosynthesis of cortisol or aldosterone, measured before or after ACTH challenge, thus demonstrating its selectivity with regard to the other enzymes involved in the steroidogenic pathway.
Glucocorticoid or mineralocorticoid replacements are therefore not needed. A non dose-dependent slight increase in serum LH and FSH levels has been observed even at low doses: this effect is, however, expected for the pharmacological class and is probably the result of feedback at the pituitary level due to the reduction in oestrogen levels that stimulate the pituitary secretion of gonadotropins also in postmenopausal women.
Adjuvant treatment of early breast cancer: In a multicentre, randomised, double-blind study, conducted in 4,724 postmenopausal patients with oestrogen-receptor-positive or unknown primary breast cancer, patients who had remained disease-free after receiving adjuvant tamoxifen therapy for 2 to 3 years were randomised to receive 3 to 2 years of exemestane (25 mg/day) or tamoxifen (20 or 30 mg/day) to complete a total of 5 years of hormonal therapy.
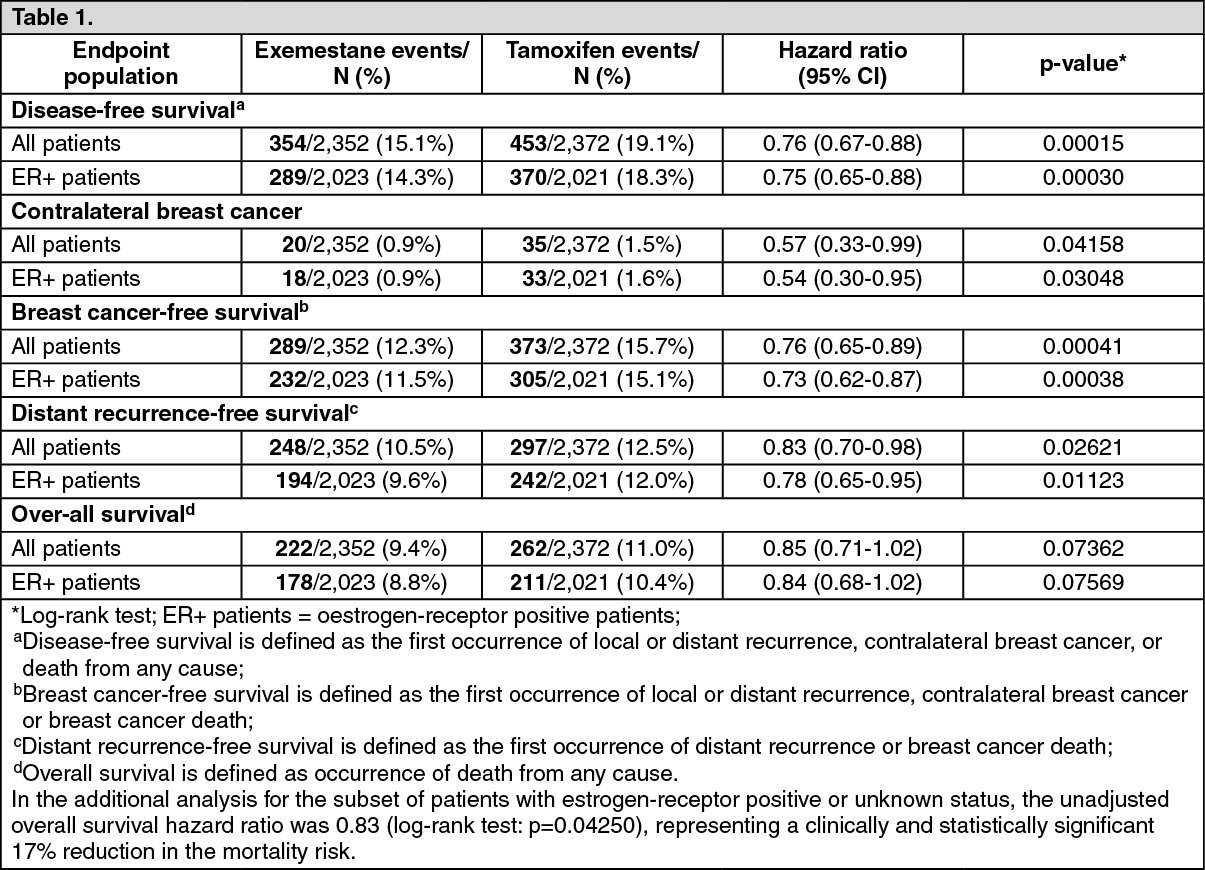
After a median duration of therapy of about 30 months and a median follow-up of about 52 months, results showed that sequential treatment with exemestane after 2 to 3 years of adjuvant tamoxifen therapy was associated with a clinically and statistically significant improvement in disease-free survival (DFS) compared with continuation of tamoxifen therapy. Analysis showed that, in the observed study period, exemestane reduced the risk of breast cancer recurrence by 24% compared with tamoxifen (hazard ratio 0.76; p=0.00015). The beneficial effect of exemestane over tamoxifen with respect to DFS was apparent regardless of nodal status or prior chemotherapy.
Exemestane also significantly reduced the risk of contralateral breast cancer (hazard ratio 0.57, p=0.04158).
In the whole study population, a trend for improved overall survival was observed for exemestane (222 deaths) compared to tamoxifen (262 deaths) with a hazard ratio 0.85 (log-rank test: p=0.07362), representing a 15% reduction in the risk of death in favour of exemestane. A statistically significant 23% reduction in the mortality risk (hazard ratio for overall survival 0.77; Wald chi square test: p=0.0069) was observed for exemestane compared to tamoxifen when adjusting for the pre-specified prognostic factors (i.e. ER status, nodal status, prior chemotherapy, use of HRT and use of bisphosphonates).
Main efficacy outcomes in all patients (intention-to-treat population) and oestrogen-receptor positive patients are summarised in the table as follows: (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageResults from a bone substudy demonstrated that women treated with exemestane following 2 to 3 years of tamoxifen treatment experienced a moderate reduction in bone mineral density. In the overall study, the treatment-emergent fracture incidence evaluated during the 30-month treatment period was higher in patients treated with exemestane compared with tamoxifen (4.5% and 3.3% respectively, p=0.038).
Results from an endometrial substudy indicate that, after 2 years of treatment, there was a median 33% reduction in endometrial thickness among the exemestane-treated patients compared with no notable variation in the tamoxifen-treated patients. Endometrial thickening, reported at the start of study treatment, was reversed to normal (<5 mm) for 54% of patients treated with exemestane.
Treatment of advanced breast cancer: In a randomised, peer-reviewed, controlled clinical trial, exemestane at the daily dose of 25 mg has demonstrated statistically significant prolongation of survival, Time to Progression (TTP) and Time to Treatment Failure (TTF), as compared to a standard hormonal treatment with megestrol acetate in postmenopausal patients with advanced breast cancer that had progressed following or during treatment with tamoxifen, either as adjuvant therapy or as first line treatment for advanced disease.
Pharmacokinetics: Absorption: After oral administration of exemestane tablets, exemestane is rapidly absorbed. The fraction of the dose absorbed from the gastrointestinal tract is high. Absolute bioavailability in humans is unknown, although it is anticipated to be limited by an extensive first-pass effect. A similar effect resulted in an absolute bioavailability in rats and dogs of 5%. After a single dose of 25 mg, maximum plasma levels of 18 ng/mL are reached after 2 hours. Concomitant intake with food increases the bioavailability by 40%.
Distribution: The volume of distribution of exemestane, not corrected for oral bioavailability, is about 20,000 L. The kinetics is linear and the terminal elimination half-life is 24 h. Binding to plasma proteins is 90% and is concentration-independent. Exemestane and its metabolites do not bind to red blood cells.
Exemestane does not accumulate in an unexpected way after repeated dosing.
Metabolism and excretion: Exemestane is metabolised by oxidation of the methylene moiety on the 6-position by CYP3A4 isoenzyme and/or reduction of the 17-keto group by aldoketoreductase followed by conjugation. The clearance of exemestane is about 500 L/h, not corrected for oral bioavailability.
The metabolites are inactive or inhibition of aromatase is less than the parent compound. The amount excreted unchanged in urine is 1% of the dose. In urine and faeces, equal amounts (40%) of 14C-labelled exemestane were eliminated within one week.
Special populations: Age: No significant correlation between the systemic exposure of exemestane and the age of subjects has been observed.
Renal insufficiency: In patients with severe renal impairment (CLcr <30 mL/min), the systemic exposure to exemestane was 2 times higher compared with healthy volunteers.
Given the safety profile of exemestane, no dose adjustment is considered necessary.
Hepatic insufficiency: In patients with moderate or severe hepatic impairment, the exposure of exemestane is 2-3 fold higher compared with healthy volunteers. Given the safety profile of exemestane, no dose adjustment is considered necessary.
Toxicology: Preclinical safety data: Toxicological studies: Findings in the repeat-dose toxicology studies in rat and dog were generally attributable to the pharmacological activity of exemestane, such as effects on reproductive and accessory organs. Other toxicological effects (on liver, kidney or central nervous system) were observed only at exposures considered sufficiently in excess of the maximum human exposure, indicating little relevance to clinical use.
Mutagenicity: Exemestane was not genotoxic in bacteria (Ames test), V79 Chinese hamster cells, rat hepatocytes or in the mouse micronucleus assay. Although exemestane was clastogenic in lymphocytes in vitro, it was not clastogenic in two in vivo studies.
Reproductive toxicology: Exemestane was embryotoxic in rats and rabbits at systemic exposure levels similar to those obtained in humans at 25 mg/day. There was no evidence of teratogenicity.
Carcinogenicity: In a two-year carcinogenicity study in female rats, no treatment-related tumours were observed. In male rats, the study was terminated in week 92 due to early death by chronic nephropathy. In a two-year carcinogenicity study in mice, an increase in the incidence of hepatic neoplasms in both genders was observed at the intermediate and high doses (150 and 450 mg/kg/day). This finding is considered to be related to the induction of hepatic microsomal enzymes, an effect observed in mice but not in clinical studies. An increase in the incidence of renal tubular adenomas was also noted in male mice at the high dose (450 mg/kg/day). This change is considered to be species- and gender-specific, occurring at a dose which represents 63-fold greater exposure than with the human therapeutic dose. None of these observed effects is considered to be clinically relevant to the treatment of patients with exemestane.