


 Sign Out
Sign Out
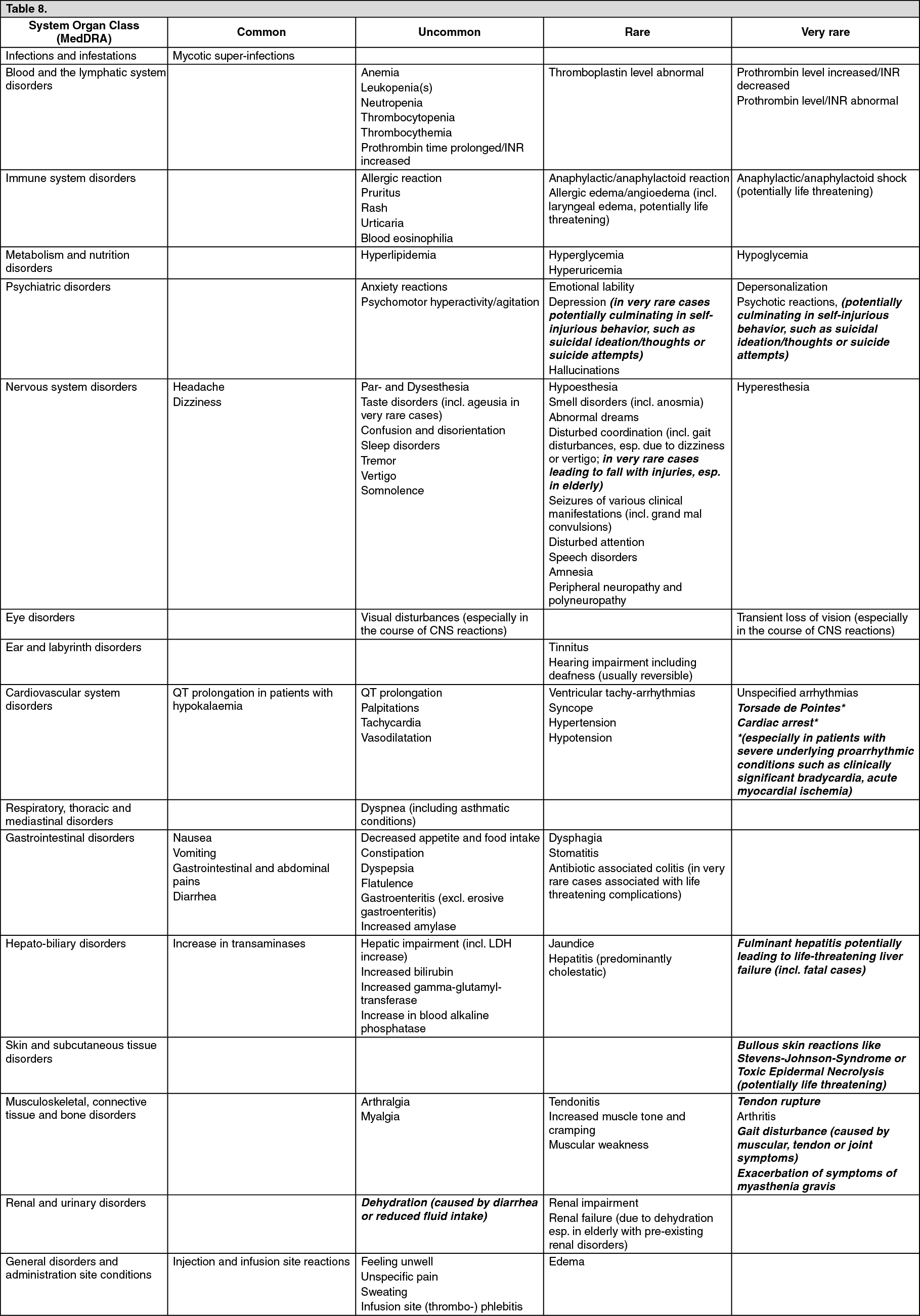
ADRs derived from post marketing reports (status: May 2010) are printed in bold italic.
Within each frequency grouping, undesirable effects are presented in order of decreasing seriousness. Frequencies are defined as: common (≥ 1/100 to < 1/10), uncommon (≥ 1/1,000 to < 1/100), rare (≥ 1/10,000 to < 1/1,000), very rare (< 1/10,000). (See Table 8.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn isolated instances, some serious adverse drug reactions may be long-lasting (> 30 days) and disabling; such as tendinitis, tendon rupture, musculoskeletal disorders, and other reactions affecting the nervous system including psychiatric disorders and disturbance of senses.
The following undesirable effects have a higher frequency in the subgroup of IV/oral sequentially treated patients: Common: Increased gamma-glutamyl-transferase.
Uncommon: Ventricular tachyarrhythmias, Hypotension, Edema, Antibiotic associated colitis (in very rare cases associated with life threatening complications), Seizures of various clinical manifestations (incl. grand mal convulsions), Hallucinations, Renal impairment and Renal failure (due to dehydration esp. in elderly with pre-existing renal disorders).
Additional information on special populations: Pediatric patients: Adverse reactions in children (>3 months - <18 years) were derived from a clinical study in pediatric patients with complicated intra-abdominal infection. For the safety analysis, data from a total of 301 pediatric patients treated with moxifloxacin were available, thereof 15 patients below the age of 6 years and 286 patients at the age of 6 - <18 years.
Cartilage damage of weight-bearing joints in juvenile animals is a known class effect of fluoroquinolones. Therefore, musculoskeletal events were carefully monitored and followed up over 1 year after the study treatment. The musculoskeletal adverse events observed in the study were mostly rated as mild in intensity, and were equally distributed among the moxifloxacin and the comparator groups. There were no events indicating chondropathy.
Moxifloxacin has been shown to prolong the QT interval of the electrocardiogram in some patients (see Precautions). The ECG analyses in pediatric patients revealed that QT prolongation is common. No cardiovascular morbidity or mortality attributable to QTc prolongation occurred with moxifloxacin treatment in the pediatric study. For specific warnings and precautions for use referring to QT prolongation, see Special warnings and precautions for use.
Frequency, type and severity of adverse reactions in children are expected to be the same as in adults. Sub-set analyses by age groups did not reveal any age-related exceptions. However, the low number of children below the age of 6 years limits the analysis of adverse reactions in younger children.
View ADR Monitoring Form