Posology: For all indications a titration scheme for the initiation of therapy is described in Table 3, which is recommended for adults and adolescents aged 12 years and above. Dosing instructions for children under 12 years of age are provided under a separate sub-heading as follows. (See Table 3.)
 Click on icon to see table/diagram/image
Discontinuation of gabapentin:
Click on icon to see table/diagram/image
Discontinuation of gabapentin: In accordance with current clinical practice, if gabapentin has to be discontinued it is recommended this should be done gradually over a minimum of 1 week independent of the indication.
Epilepsy: Epilepsy typically requires long-term therapy. Dosage is determined by the treating physician according to individual tolerance and efficacy.
Adults and adolescents: In clinical trials, the effective dosing range was 900 to 3600 mg/day. Therapy may be initiated by titrating the dose as described in Table 2 or by administering 300 mg three times a day (TID) on Day 1. Thereafter, based on individual patient response and tolerability, the dose can be further increased in 300 mg/day increments every 2-3 days up to a maximum dose of 3600 mg/day. Slower titration of gabapentin dosage may be appropriate for individual patients. The minimum time to reach a dose of 1800 mg/day is one week, to reach 2400 mg/day is a total of 2 weeks, and to reach 3600 mg/day is a total of 3 weeks. Dosages up to 4800 mg/day have been well tolerated in long-term open-label clinical studies. The total daily dose should be divided in three single doses, the maximum time interval between the doses should not exceed 12 hours to prevent breakthrough convulsions.
Children aged 6 years and above: The starting dose should range from 10 to 15 mg/kg/day and the effective dose is reached by upward titration over a period of approximately three days. The effective dose of gabapentin in children aged 6 years and older is 25 to 35 mg/kg/day. Dosages up to 50 mg/kg/day have been well tolerated in a long-term clinical study. The total daily dose should be divided in three single doses, the maximum time interval between doses should not exceed 12 hours.
It is not necessary to monitor gabapentin plasma concentrations to optimize gabapentin therapy. Further, gabapentin may be used in combination with other antiepileptic medicinal products without concern for alteration of the plasma concentrations of gabapentin or serum concentrations of other antiepileptic medicinal products.
Peripheral neuropathic pain: Adults: The therapy may be initiated by titrating the dose as described in Table 3. Alternatively, the starting dose is 900 mg/day given as three equally divided doses. Thereafter, based on individual patient response and tolerability, the dose can be further increased in 300 mg/day increments every 2-3 days up to a maximum dose of 3600 mg/day. Slower titration of gabapentin dosage may be appropriate for individual patients. The minimum time to reach a dose of 1800 mg/day is one week, to reach 2400 mg/day is a total of 2 weeks, and to reach 3600 mg/day is a total of 3 weeks.
In the treatment of peripheral neuropathic pain such as painful diabetic neuropathy and post-herpetic neuralgia, efficacy and safety have not been examined in clinical studies for treatment periods longer than 5 months. If a patient requires dosing longer than 5 months for the treatment of peripheral neuropathic pain, the treating physician should assess the patient's clinical status and determine the need for additional therapy.
Instruction for all areas of indication: In patients with poor general health, i.e., low body weight, after organ transplantation etc., the dose should be titrated more slowly, either by using smaller dosage strengths or longer intervals between dosage increases.
Elderly (over 65 years of age): Elderly patients may require dosage adjustment because of declining renal function with age (see Table 4). Somnolence, peripheral oedema and asthenia may be more frequent in elderly patients.
Renal impairment: Dosage adjustment is recommended in patients with compromised renal function as described in Table 4 and/or those undergoing haemodialysis. Gabapentin 100 mg capsules can be used to follow dosing recommendations for patients with renal insufficiency. (See Table 4.)
Click on icon to see table/diagram/image
Use in patients undergoing haemodialysis: For anuric patients undergoing haemodialysis who have never received gabapentin, a loading dose of 300 to 400 mg, then 200 to 300 mg of gabapentin following each 4 hours of haemodialysis, is recommended. On dialysis-free days, there should be no treatment with gabapentin.
For renally impaired patients undergoing haemodialysis, the maintenance dose of gabapentin should be based on the dosing recommendations found in Table 4. In addition to the maintenance dose, an additional 200 to 300 mg dose following each 4-hour haemodialysis treatment is recommended.
Method of administration: For oral use. Gabapentin can be given with or without food and should be swallowed whole with sufficient fluid-intake (e.g. a glass of water).


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image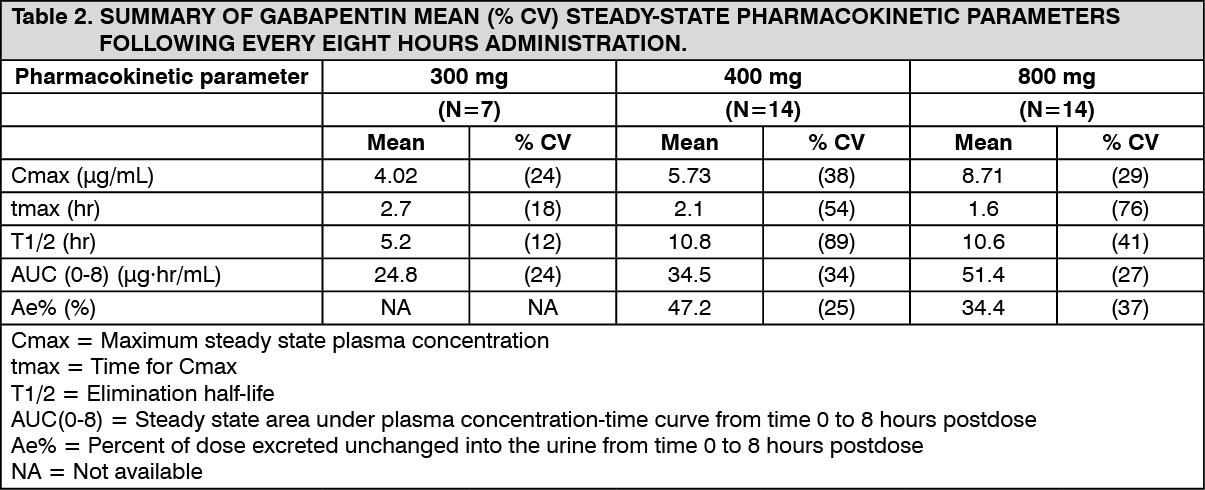 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image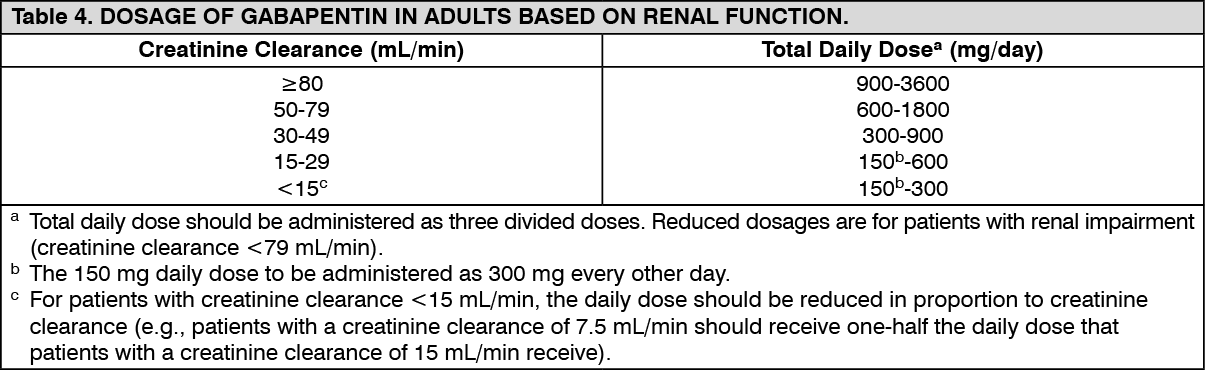 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out