


 Sign Out
Sign Out

In studies of patients with mCSPC (TITAN) or nmCRPC (SPARTAN) who were using a GnRH analog, or were previously treated with orchiectomy, Apalutamide (Erleada) was administered at a dose of 240 mg daily.
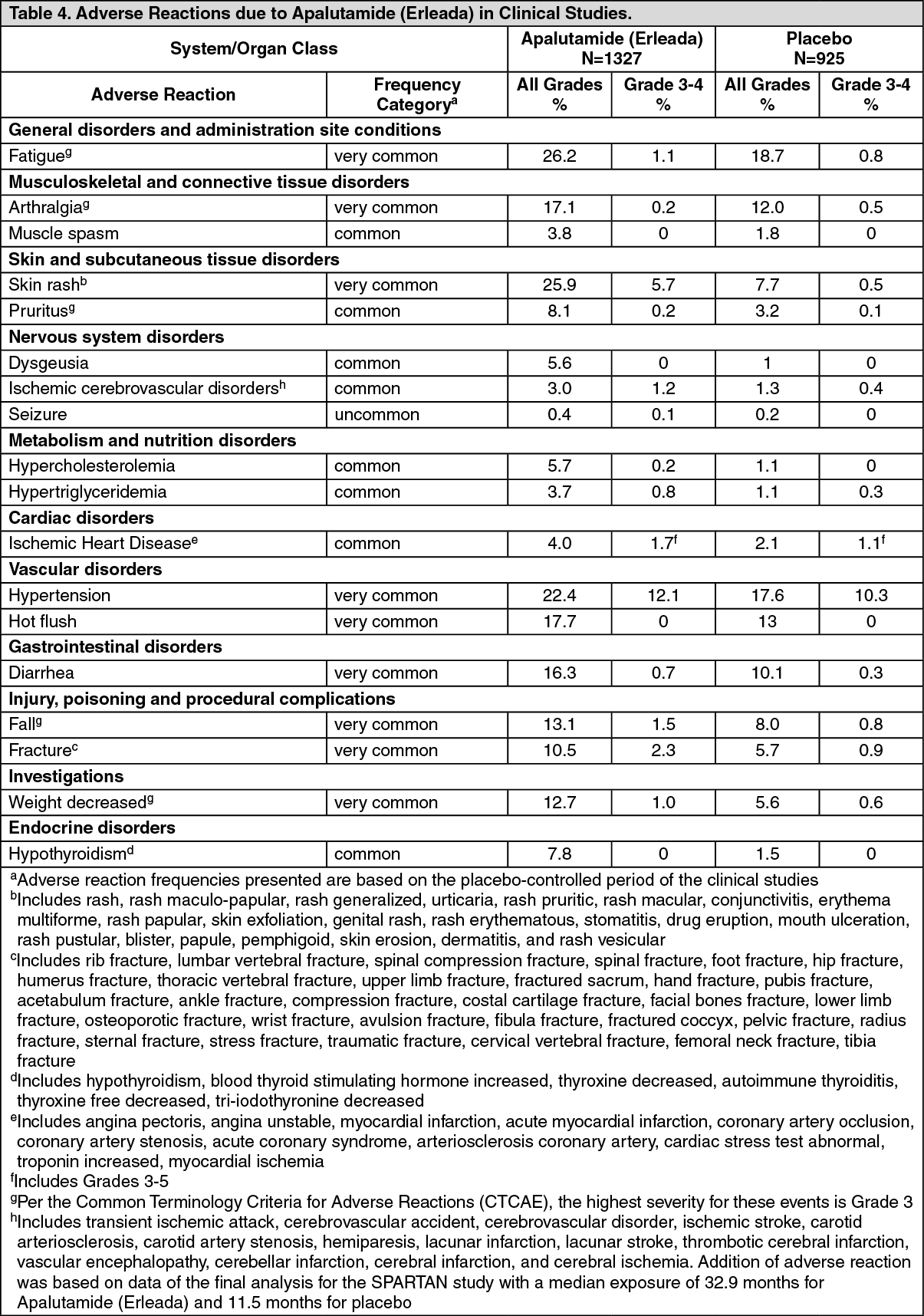
Table 4 shows adverse reactions on the Apalutamide (Erleada) arm in the combined data that occurred with a ≥2% absolute increase in frequency compared to placebo or were events of special interest. ARs are also listed by system organ class and frequency: very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1000 to < 1/100), and rare (≥ 1/10000 to < 1/1000). Within each frequency grouping, ARs are presented in order of decreasing frequency. (See Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSkin rash: In the combined data of two randomized, placebo-controlled clinical studies, skin rash associated with Apalutamide (Erleada) was most commonly described as macular or maculo-papular. Adverse reactions of skin rash were reported for 26% of subjects treated with Apalutamide (Erleada) versus 8% of subjects treated with placebo. Grade 3 skin rashes (defined as covering > 30% body surface area [BSA]) were reported with Apalutamide (Erleada) treatment (6%) versus placebo (0.5%). There were no reported events of toxic epidermal necrolysis (TEN) or Stevens-Johnson syndrome (SJS) in clinical trials.
The onset of skin rash occurred at a median of 83 days of Apalutamide (Erleada) treatment and resolved within a median of 78 days from onset of rash for 78% of subjects. Rash was commonly managed with oral antihistamines, topical corticosteroids, and 19% of subjects received systemic corticosteroids. Among subjects with skin rash, dose interruption occurred in 28% and dose reduction occurred in 14% (see Dose modification under Dosage & Administration). Of the patients who had dose interruption, 59% experienced recurrence of rash upon reintroduction of Apalutamide (Erleada). Skin rash led to Apalutamide (Erleada) treatment discontinuation in 7% of subjects who experienced skin rash.
Hypothyroidism: In the combined data of two randomized, placebo-controlled studies, hypothyroidism was reported for 8% of subjects treated with Apalutamide (Erleada) and 2% of subjects treated with placebo based on assessments of thyroid-stimulating hormone (TSH) every 4 months. There were no grade 3 or 4 adverse reactions. Hypothyroidism occurred in 30% of subjects already receiving thyroid replacement therapy in the Apalutamide (Erleada) arm and in 3% of subjects in the placebo arm. In subjects not receiving thyroid replacement therapy, hypothyroidism occurred in 7% of subjects treated with Apalutamide (Erleada) and in 2% of subjects treated with placebo. Thyroid replacement therapy, when clinically indicated, should be initiated or dose-adjusted (see Effect of Apalutamide (Erleada) on drug metabolizing enzymes under Interactions).
Postmarketing data: In addition to the adverse reactions reported during clinical studies and listed previously, the following adverse reactions have been reported during postmarketing experience (Table 5). Because these reactions were reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure. In the table, the frequencies are provided according to the following convention: Very common ≥ 1/10 (≥ 10%), Common ≥ 1/100 and < 1/10 (≥ 1% and < 10%), Uncommon ≥ 1/1000 and < 1/100 (≥ 0.1% and < 1%), Rare ≥ 1/10000 and < 1/1000 (≥ 0.01 and < 0.1%), Very rare < 1/10000, including isolated reports (< 0.01%), Not known Cannot be estimated from the available data.
In Table 5, adverse reactions are presented by frequency category based on spontaneous reporting rates and by frequency category based on incidence in clinical trials or epidemiology studies, when known. (See Table 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
View ADR Monitoring Form