Esomeprazole should not be administered concomitantly with any other medications through the same intravenous site and or tubing. The intravenous line should always be flushed with either 0.9% Sodium Chloride Injection, USP, Lactated Ringer's Injection, USP or 5% Dextrose Injection, USP both prior to and after administration of Esomeprazole.
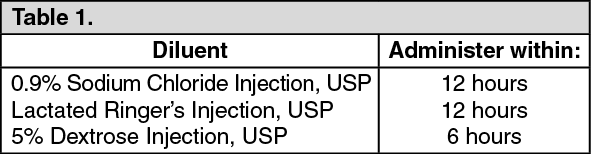
The admixture should be stored at room temperature up to 30°C (86°F) and should be administered within the designated time period as listed in the Table 1 as follows. No refrigeration is required. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit.
As soon as oral therapy is possible or appropriate, intravenous therapy with Esomeprazole discontinued and the therapy should be continued orally.
GERD with Erosive Esophagitis: Adults: The recommended adult dose is either 20 mg or 40 mg esomeprazole given once daily by intravenous injection (no less than 3 minutes) or intravenous infusion (10 minutes to 30 minutes). Safety and efficacy of Esomeprazole as a treatment of GERD patients with erosive esophagitis for more than 10 days have not been demonstrated.
Pediatric: The recommended doses for children ages 1 month to 17 years, inclusive, are provided as follows. Dose should be infused over 10 minutes to 30 minutes.
1 year to 17 years: Body weight less than 55 kg: 10 mg.
Body weight 55 kg or greater: 20 mg.
1 month to less than 1 year of age: 0.5 mg/kg.
Administration: Adults: Intravenous Injection (20 mg or 40 mg vial) over no less than 3 minutes. The freeze-dried powder should be reconstituted with 5 mL of 0.9% Sodium Chloride Injection, USP. Withdraw 5 mL of the reconstituted solution and administer an intravenous injection over no less than 3 minutes. Intravenous Infusion (20 mg or 40 mg) over 10 minutes to 30 minutes, a solution for intravenous infusion is prepared by first reconstituting the contents of one vial with 5 mL of 0.9% Sodium Chloride Injection, USP, Lactated Ringer's Injection, USP or 5% Dextrose Injection, USP and further diluting the resulting solution to a final volume of 50 mL. The solution (admixture) should be administered as an intravenous infusion over a period of 10 minutes to 30 minutes. The reconstituted solution should be stored at room temperature up to 30°C (86°F) and administered within 12 hours after reconstitution. No refrigeration is required.
Pediatric Population: Intravenous Infusion over 10 minutes to 30 minutes (0.5 mg/kg) for patients ages 1 month to less than 1 year of age. A solution for intravenous infusion is prepared by first reconstituting the contents of one vial with 5 mL of 0.9% Sodium Chloride Injection, USP and further diluting the resulting solution to a final volume of 50 mL. The resultant concentration after diluting to a final volume of 50 mL is as: 40 mg vial: 0.8 mg/mL.
Withdraw appropriate amount of volume for desired dose (0.5 mg/kg) and administer as an intravenous infusion over 10 minutes to 30 minutes.
Intravenous Infusion (10 mg and 20 mg) over 10 minutes to 30 minutes for Pediatric Patients, ages 1 year to 17 years of age 40 mg vial. A solution for intravenous infusion is prepared by first reconstituting the contents of one vial with 5 mL of 0.9% Sodium Chloride Injection, USP and further diluting the resulting solution to a final volume of 50 mL. The resultant concentration after diluting to a final volume of 50 mL is 0.8 mg/mL.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out