Clinical Trials Experience: Because clinical trials are conducted under widely varying conditions, adverse event rates observed in the clinical trials of a vaccine cannot be directly compared to rates in the clinical trial of another vaccine, and may not reflect the rates observed in practice.
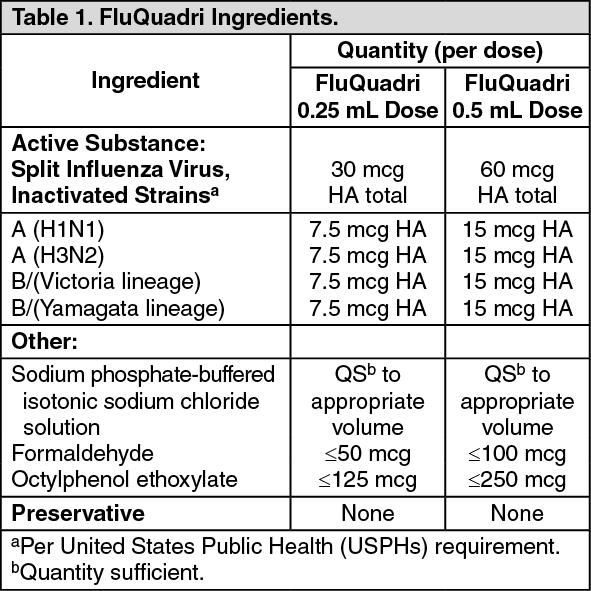
Children 6 Months through 8 Years of Age: In a multi-center study conducted in the US, children 6 months through 35 months of age received one or two 0.25 mL doses of either FluQuadri or one of two formulations of a comparator trivalent influenza vaccine (TIV-1 or TIV-2), and children 3 years through 8 years of age received one or two 0.5 mL doses of either FluQuadri, TIV-1, or TIV-2. Each of the trivalent formulations contained an influenza type B virus that corresponded to one of the two type B viruses in FluQuadri (a type B virus of the Victoria lineage or a type B virus of the Yamagata lineage). For participants who received two doses, the doses were administered approximately 4 weeks apart. The safety analysis set included 1841 children 6 months through 35 months of age and 2506 children 3 years through 8 years of age.
In children 6 months through 35 months of age, the most common (≥10%) injection-site reactions were pain (57.0%)
a or tenderness (54.1%)
b, erythema (37.3%), and swelling (21.6%); the most common solicited systemic adverse reactions were irritability (54.0%)
b, abnormal crying (41.2%)
b, malaise (38.1%)
a, drowsiness (37.7%)
b, appetite loss (32.3%)
b, myalgia (26.7%)
a, vomiting (14.8%)
b, and fever (14.3%). In children 3 years through 8 years of age, the most common (≥10%) injection-site reactions were pain (66.6%), erythema (34.1%), and swelling (24.8%); the most common solicited systemic adverse reactions were myalgia (38.6%), malaise (31.9%), and headache (23.1%).
a Assessed in children 24 months through 35 months of age.
b Assessed in children 6 months through 23 months of age.
During the 28 days following vaccination, a total of 16 (0.6%) recipients in the FluQuadri group, 4 (0.5%) recipients in the TIV-1 group, and 4 (0.6%) recipients in the TIV-2 group, experienced at least one SAE; no deaths occurred. Throughout the study period, a total of 41 (1.4%) recipients in the FluQuadri group, 7 (1.0%) recipients in the TIV-1 group, and 14 (1.9%) recipients in the TIV-2 group, experienced at least one SAE. Three SAEs were considered to be possibly related to vaccination: croup in a FluQuadri recipient and 2 episodes of febrile seizure, 1 each in a TIV-1 recipient and a TIV-2 recipient. One death occurred in the TIV-1 group (a drowning 43 days postvaccination).
Adults: In a multi-center trial conducted in the US, adults 18 years of age and older received one dose of either FluQuadri or one of two formulations of comparator trivalent influenza vaccine (TIV-1 or TIV-2). Each of the trivalent formulations contained an influenza type B virus that corresponded to one of the two type B viruses in FluQuadri (a type B virus of the Victoria lineage or a type B virus of the Yamagata lineage). The safety analysis set included 570 recipients, half aged 18-60 years and half aged 61 years or older.
In adults 18 years and older, the most common (≥10%) injection-site reaction was pain (47.4%); the most common solicited systemic adverse reactions were myalgia (23.7%), headache (15.8%), and malaise (10.5%).
In the follow-up period, there were two SAEs, 1 (0.5%) in the FluQuadri group and 1 (0.5%) in the TIV-2 group. No deaths were reported during the trial period.
Geriatric Adults: In a multi-center trial conducted in the US, adults 65 years of age and older received one dose of either FluQuadri, or one of two formulations of comparator trivalent influenza vaccine (TIV-1 or TIV-2). Each of the trivalent formulations contained an influenza type B virus that corresponded to one of the two type B viruses in FluQuadri (a type B virus of the Victoria lineage or a type B virus of the Yamagata lineage). The safety analysis set included 675 recipients.
In adults 65 years of age and older, the most common (³10%) injection-site reaction was pain (32.6%); the most common solicited systemic adverse reactions were myalgia (18.3%), headache (13.4%), and malaise (10.7%).
Three SAEs were reported during the follow-up period, 2 (0.9%) in the TIV-1 group and 1 (0.4%) in the TIV-2 group. No deaths were reported during the trial period.
Reporting adverse reactions: Persons who receive the vaccine and their guardians should be instructed to report any adverse or unusual reaction to their healthcare provider.
Post-Marketing Experience: Currently, there are no post-marketing data available for FluQuadri vaccine.
The following events have been spontaneously reported during the post-approval use of the trivalent formulation of Fluzone. Because these events are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to vaccine exposure. Adverse events were included based on one or more of the following factors: severity, frequency of reporting, or strength of evidence for a causal relationship to Fluzone.
Blood and Lymphatic System Disorders: Thrombocytopenia, lymphadenopathy.
Immune System Disorders: Anaphylaxis, other allergic/hypersensitivity reactions (including urticaria, angioedema).
Eye Disorders: Ocular hyperemia.
Nervous System Disorders: Guillain-Barré syndrome (GBS), convulsions, febrile convulsions, myelitis (including encephalomyelitis and transverse myelitis), facial palsy (Bell's palsy), optic neuritis/neuropathy, brachial neuritis, syncope (shortly after vaccination), dizziness, paresthesia.
Vascular Disorders: Vasculitis, vasodilation/flushing.
Respiratory, Thoracic and Mediastinal Disorders: Dyspnea, pharyngitis, rhinitis, cough, wheezing, throat tightness.
Skin and Subcutaneous Tissue Disorders: Stevens-Johnson syndrome.
General Disorders and Administration Site Conditions: Pruritus, asthenia/fatigue, pain in extremities, chest pain.
Gastrointestinal Disorders: Vomiting.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out