


 Sign Out
Sign Out
Pharmacology: Alfuzosin hydrochloride is an α1-adrenergic blocking agent that exhibits selectivity for α1-adrenergic receptors in the lower urinary tract (bladder base, bladder neck, prostate, prostatic capsule, prostatic urethra). Relaxation of smooth muscle in the bladder neck and prostate, which improves urine flow and reduces symptoms of benign prostatic hyperplasia (BPH), result from blockade of these adrenoceptors. Alfuzosin hydrochloride relieves moderate to severe irritative and obstructive urinary symptoms of BPH including frequency of urination, urinary urgency, nocturia, hesitancy, interrupted or weak stream, sensation of incomplete bladder emptying, and straining. These effects are generally achieved with alfuzosin hydrochloride doses without clinically important effects on blood pressure or heart rate.
Pharmacokinetics: Bioavailability: Alfuzosin hydrochloride 10 mg modified-release tablet has an absolute bioavailability of about 49% under fed conditions. It exhibits linear kinetics following single and multiple dosing of up to 30 mg.
The pharmacokinetics of a single dose of alfuzosin hydrochloride 10 mg modified-release tablet was evaluated in healthy male adult subjects under fed and fasted conditions. The following are the important pharmacokinetic parameters for the said studies: See table.
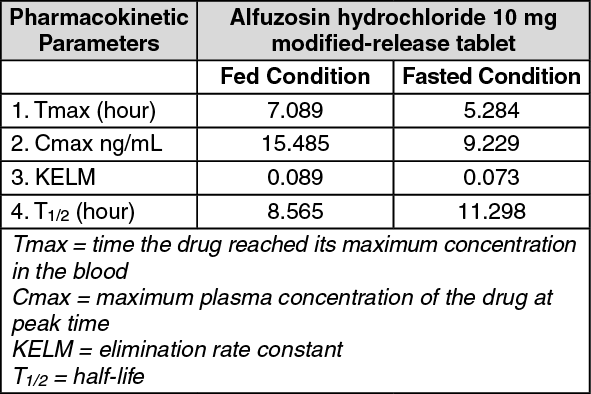 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe extent of absorption is decreased by about 50% under fasting conditions, thus, it is recommended that alfuzosin hydrochloride modified-release tablet should be taken immediately after a meal. (See DOSAGE & ADMINISTRATION).
Alfuzosin hydrochloride is about 90% bound to plasma proteins and is rapidly and extensively distributed to tissues; its volume of distribution is about 2.5 L/kg.
Alfuzosin hydrochloride is extensively metabolized with only 11% of a dose excreted unchanged in the urine. It undergoes metabolism to form inactive metabolites mainly through the liver via oxidation, O-demethylation, and/or N-dealkylation primarily through cytochrome P-450 (CYP) 3A4. It is not an inhibitor of CYP isoenzymes 1A2, 2A6, 2C9, 2C19, 2D6, or 3A4; it is also not an inducer of CYP isoenzymes 1A, 2A6, or 3A4.
Alfuzosin's apparent half-life following oral administration of a 10 mg modified-release tablet is approximately 10 hours. After 7 days, 69% and 24% of the orally administered dose of 14C-labeled alfuzosin solution were recovered in the feces and urine, respectively.
Hepatic Insufficiency: The AUC is increased and elimination half-life of alfuzosin hydrochloride is prolonged in patients with moderate to severe hepatic impairment. This results in approximately one-third to one-fourth higher plasma concentrations of alfuzosin in these patients compared to patients with normal liver function. Alfuzosin hydrochloride's pharmacokinetics has not been studied in patients with mild hepatic insufficiency.
Renal Insufficiency: Systemic alfuzosin hydrochloride exposure may increase by about 50% in patients with renal insufficiency (CLCR <80 mL/minute); safety profile appears to be the same in patients with mild (CLCR 60-80 mL/minute) or moderate (CLCR 30-59 mL/minute) renal impairment and in patients with normal renal function. Experience in patients with severe renal insufficiency is limited.