Infections and infestations: common: candidiasis (particular oral and vaginal candidiasis) or fungal infections; uncommon: vaginitis.
Blood and lymphatic system disorders: uncommon (frequency according to clinical reports: eosinophilia, leucopenia, neutropenia, thrombocytopenia.
Psychiatric disorders: uncommon: insomnia.
Nervous system disorders: common: headache, taste perversiona (metallic aftertaste); uncommon: dizziness, hypesthesia, paresthesia.
Eye disorders: uncommon: visual loop.
Ear disorders: uncommon: tinnitus.
Cardiovascular disorders: uncommon: arterial hypertension, phlebitis/thrombophlebitis.
Digestive tract disorders: common: diarrhea, nausea, vomiting; uncommon: local and general abdominal pain, constipation, dry mouth, dyspepsia, gastritis, glossitis, abnormal stool, pancreatitis, stomatitis, change in tongue color.
Hepatobiliary disorders: common: abnormal liver function tests.
Skin and subcutaneous tissue disorders: uncommon: dermatitis, hyperhidrosis, itching, rash, urticaria.
Urinary disorders: uncommon: polyuria.
Reproductive and breast disorders: uncommon: vulvovaginal disorders.
General disorders and administration site conditions: uncommon: fever, fatigue, pain at injection site, dipsosis, local pain.
Laboratory findings: Biochemistry: common: increase AST, ALT, LDH, alkaline phosphatase, blood urea nitrogen, creatine phosphokinase, lipase, amylase or glucose without starvation; decrease in total protein, albumin, sodium and calcium; increase of decrease of potassium or bicarbonate; uncommon: increase in total bilirubin, creatinine, sodium and calcium; decrease in glucose without starvation; increase of decrease of chlorides.
Haematology: common: increase in neutrophil and eosinophil counts; decrease in hemoglobin, hematocrit or erythrocytes count; increase of decrease of platelet or leucocyte counts; uncommon: increase in reticulocyte count; decrease in neutrophil count.
The following side reactions were evaluated as serious in isolated cases: localized abdominal pain, transient ischemic attacks, arterial hypertension, pancreatitis and renal failure.
During clinical studies, one case of drug-induced arrhythmia (tachycardia) was reported.
In controlled clinical studies in which Linezolid was given for a period up to 28 days, anemia was reported in less than 0.1% of patients. In treatment program for patients with life-threatening infections and concurrent diseases, rate of patients with anemia developed under administration of Linezolid within <28 days was 2.5%, as compared to 12.3%, when treatment lasted for >28 days.
Post-marketing experience: Blood and lymphatic system disorders: anemia, leukopenia, neutropenia, thrombocytopenia, pancytopenia and myelosuppression. In case of anemia developing, more patients needed hemotransfusion under treatment with Linezolid for a period longer than recommended 28 days.
Immune system disorders: anaphylaxis; trophic and metabolic disorders: lactate acidosis.
Nervous system disorders: peripheral neuropathy, seizures, serotonin syndrome. Peripheral neuropathy was reported among patients receiving Linezolid. These reports concern primarily the patients receiving drug for a period longer than recommended 28 days.
Seizures were reported among patients receiving Linezolid. In most cases, there were seizures or factors of seizure occurrence risk in history of patients.
Cases of serotonin syndrome were reported.
Eye disorders: optic neuropathy, sometimes progressing to loss of vision (cases were primarily observed in patients receiving drug for a period longer than recommended 28 days).
Skin and subcutaneous tissue disorders: angioedema, skin blisters, such as Stevens-Johnson syndrome.



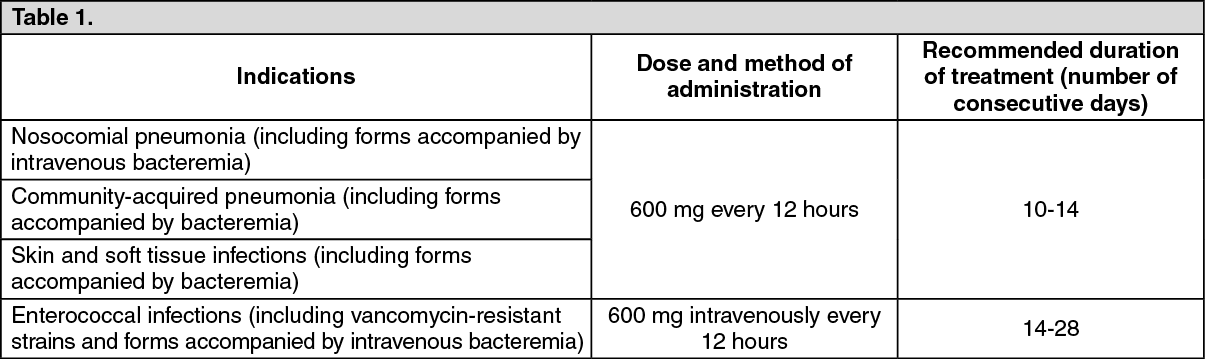 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image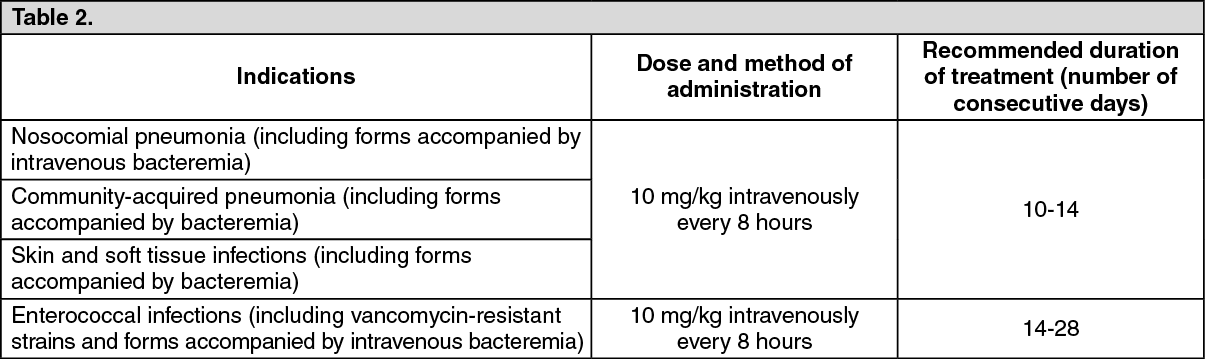 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out