


 Sign Out
Sign Out
Therapy with drugs that are predominantly metabolized by the CYP2D6 system and have a relatively narrow therapeutic index (e.g., flecainide, propafenone, vinblastine, and TCAs) should be initiated at the low end of the dose range if a patient is receiving fluoxetine concurrently or has taken it in the previous five weeks. Thus, the patient's dosing requirements resemble those of poor metabolizers. (see Interactions)
Fluoxetine should be administered orally, with or without food.
Fluoxetine in combination with olanzapine should be administered once a day in the evening, without regard to meals.
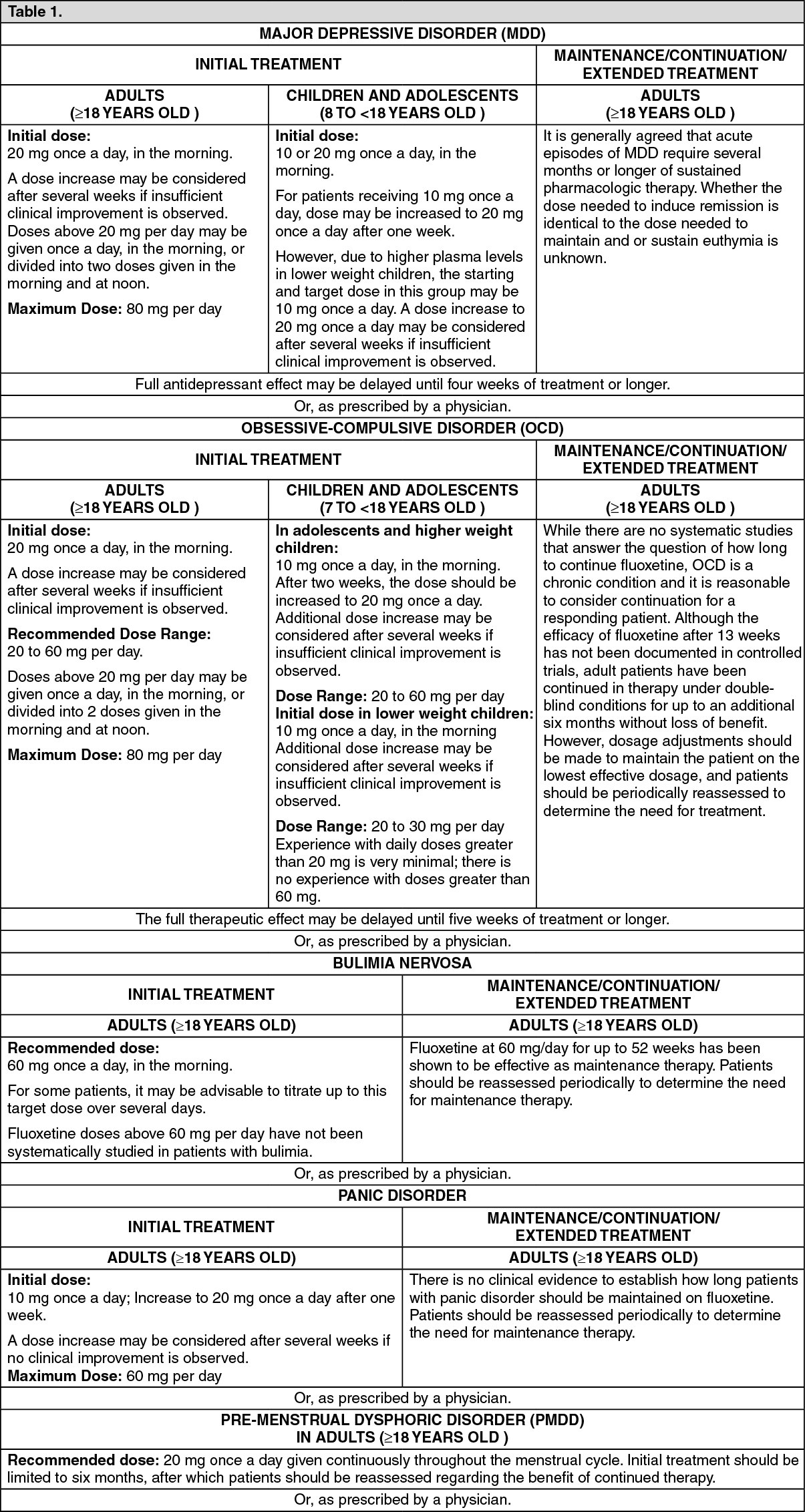
Recommended Oral Fluoxetine Dose: See Table 1.
 Click on icon to see table/diagram/image
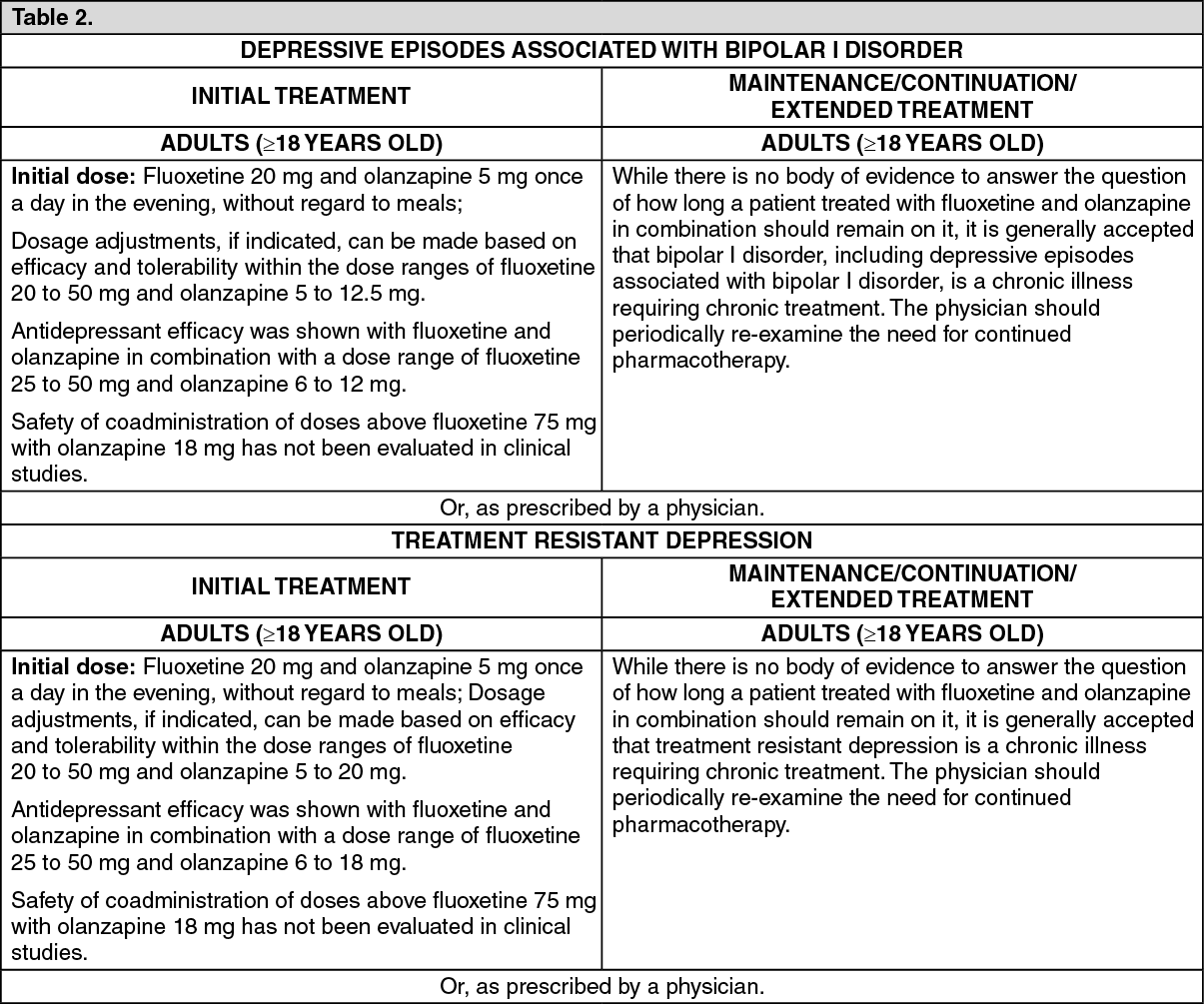
Click on icon to see table/diagram/imageFluoxetine in Combination with Oral Olanzapine: See Table 2.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageFluoxetine in Combination with Olanzapine Dosing in Special Population: Patients with a predisposition to hypotensive reactions, patients with hepatic impairment, or patients who exhibit a combination of factors that may slow the metabolism of fluoxetine or olanzapine in combination (female gender, geriatric age, non-smoking status), or those patients who may be.
pharmacodynamically sensitive to olanzapine: Recommended starting dose: Fluoxetine 20 mg and olanzapine 2.5 to 5 mg; Dose modifications may be necessary in patients who exhibit a combination of factors that may slow metabolism.
When indicated, dose escalation should be done with caution in these patients.
Fluoxetine and olanzapine in combination have not been systematically studied in patients 65 years and older or in patients below 18 years old.
Discontinuation of Fluoxetine: There have been spontaneous reports of adverse reactions occurring upon discontinuation of fluoxetine, selective norepinephrine reuptake inhibitors (SNRIs), and selective serotonin reuptake inhibitors (SSRIs), particularly when abrupt, such as dysphonic mood, irritability, agitation, dizziness, sensory disturbances (e.g., paresthesia such as electric shock sensations), anxiety, confusion, headache, lethargy, emotional lability, insomnia, and hypomania. While these reactions are generally self-limiting, there have been reports of serious discontinuation symptoms. Patients should be monitored for these symptoms when discontinuing treatment. A gradual reduction in the dose rather than abrupt cessation is recommended whenever possible. If intolerable symptoms occur following a decrease in the dose or upon discontinuation of treatment, then resuming the previously prescribed dose may be considered. Subsequently, the physician may continue decreasing the dose but with a more gradual rate. Plasma fluoxetine and norfluoxetine concentration decrease gradually at the conclusion of therapy which may minimize the risk of discontinuation symptoms with this drug.