Body as a Whole: Chills, chills and fever, face edema, intentional injury, fever, flu syndrome, asthenia, malaise, hypothermia.
Cardiovascular System: Vasodilation, hemorrhage, hypertension, palpitation, angina pectoris, arrhythmia, congestive heart failure, hypotension, myocardial infarction, chest pain, postural hypotension, syncope, tachycardia, vascular headache, atrial fibrillation, bradycardia, cerebral embolism, cerebral ischemia, cerebrovascular accident, extrasystoles, heart arrest, heart block, pallor, peripheral vascular disorder, phlebitis, shock, thrombophlebitis, thrombosis, vasospasm, ventricular arrhythmia, ventricular extrasystoles, ventricular fibrillation.
Digestive System: Constipation, diarrhea, dry mouth, dyspepsia, flatulence, nausea, vomiting, aphthous stomatitis, cholelithiasis, colitis, dysphagia, eructation, esophagitis, gastritis, gastroenteritis, glossitis, gum hemorrhage, hyperchlorhydria, increased salivation, abnormal liver function tests, melena, mouth ulceration, nausea/vomiting/diarrhea, stomach ulcer, stomatitis, thirst, biliary pain, bloody diarrhea, cholecystitis, duodenal ulcer, enteritis, esophageal ulcer, fecal incontinence, gastrointestinal hemorrhage, hematemesis, colon hemorrhage, hepatitis, intestinal obstruction, liver fatty deposit, pancreatitis, peptic ulcer, rectal hemorrhage, salivary gland enlargement, stomach ulcer hemorrhage, tongue edema, acute abdominal syndrome.
Hemic and Lymphatic System: Anemia, ecchymosis, blood dyscrasia, hypochromic anemia, leukopenia, lymphedema, lymphocytosis, petechia, purpura, thrombocythemia, thrombocytopenia.
Metabolic/Endocrine and Nutritional Disorders: Anorexia, weight loss, weight gain, increased appetite, dehydration, generalized edema, gout, hypercholesterolemia, hyperlipemia, hypokalemia, peripheral edema, alcohol intolerance, increased alkaline phosphatase, increased BUN, increased creatine phosphokinase, hyperkalemia, hyperuricemia, hypocalcemia, iron deficiency anemia, increased ALT, hyponatremia, hypothyroidism, diabetic acidosis, diabetes mellitus, decreased/increased libido, impotence, sexual dysfunction, priapism, galactorrhea.
Musculoskeletal System: Arthritis, bone pain, bone fractures, bursitis, leg cramps, tenosynovitis, arthrosis, chondrodystrophy, myasthenia, myopathy, myositis, osteomyelitis, osteoporosis, rheumatoid arthritis, arthralgia, myalgia, pelvic pain.
Nervous System: Abnormal dreams, abnormal thinking, anxiety, dizziness, nervousness, somnolence, tremor, insomnia, agitation, amnesia, confusion, emotional lability, sleep disorder, abnormal gait, acute brain syndrome, akathisia, apathy, ataxia, buccoglossal syndrome, CNS depression, CNS stimulation, depersonalization, euphoria, hallucinations, hostility, hyperkinesia, hypertonia, hypoesthesia, incoordination, myoclonus, neuralgia, neuropathy, neurosis, paranoid reaction, personality disorder, psychosis, vertigo, abnormal electroencephalogram, antisocial reaction, circumoral paresthesia, coma, delusions, dysarthria, dystonia, extrapyramidal syndrome, foot drop, hyperesthesia, neuritis, paralysis, decreased/increased reflexes, stupor, headache, migraine, neuroleptic malignant syndrome-like events, suicidal ideation.
Respiratory System: Pharyngitis, sinusitis, yawn, asthma, epistaxis, hiccups, hyperventilation, apnea, atelectasis, decreased cough, emphysema, hemoptysis, hypoventilation, hypoxia, larynx edema, lung edema, pneumothorax, stridor, dyspnea.
Skin and Appendages: Sweating, pruritus, rash, urticaria, anaphylactoid reaction, vasculitis, angioedema, serum sickness-like reaction, acne, alopecia, contact dermatitis, eczema, maculopapular rash, skin discoloration, skin ulcer, vesiculobullous rash, furunculosis, herpes zoster, hirsutism, petechial rash, psoriasis, purpuric rash, pustular rash, seborrhea, Stevens-Johnson syndrome, toxic epidermal necrolysis, erythema multiforme, photosensitivity reaction.
Special Senses: Abnormal vision, conjunctivitis, dry eyes, mydriasis, photophobia, blepharitis, diplopia, exophthalmos, eye hemorrhage, glaucoma, hyperacusis, iritis, parosmia, scleritis, strabismus, visual field defect, ear pain, tinnitus, taste perversion, taste loss.
Urogenital System: Abnormal ejaculation, urinary frequency, abortion, albuminuria, amenorrhea, anorgasmia, breast enlargement, breast pain, cystitis, dysuria, female lactation, fibrocystic breast, hematuria, leukorrhea, menorrhagia, metrorrhagia, nocturia, polyuria, urinary incontinence, urinary retention, urinary urgency, vaginal hemorrhage, breast engorgement, glycosuria, hypomenorrhea, kidney pain, oliguria, uterine hemorrhage, uterine fibroids enlargement.


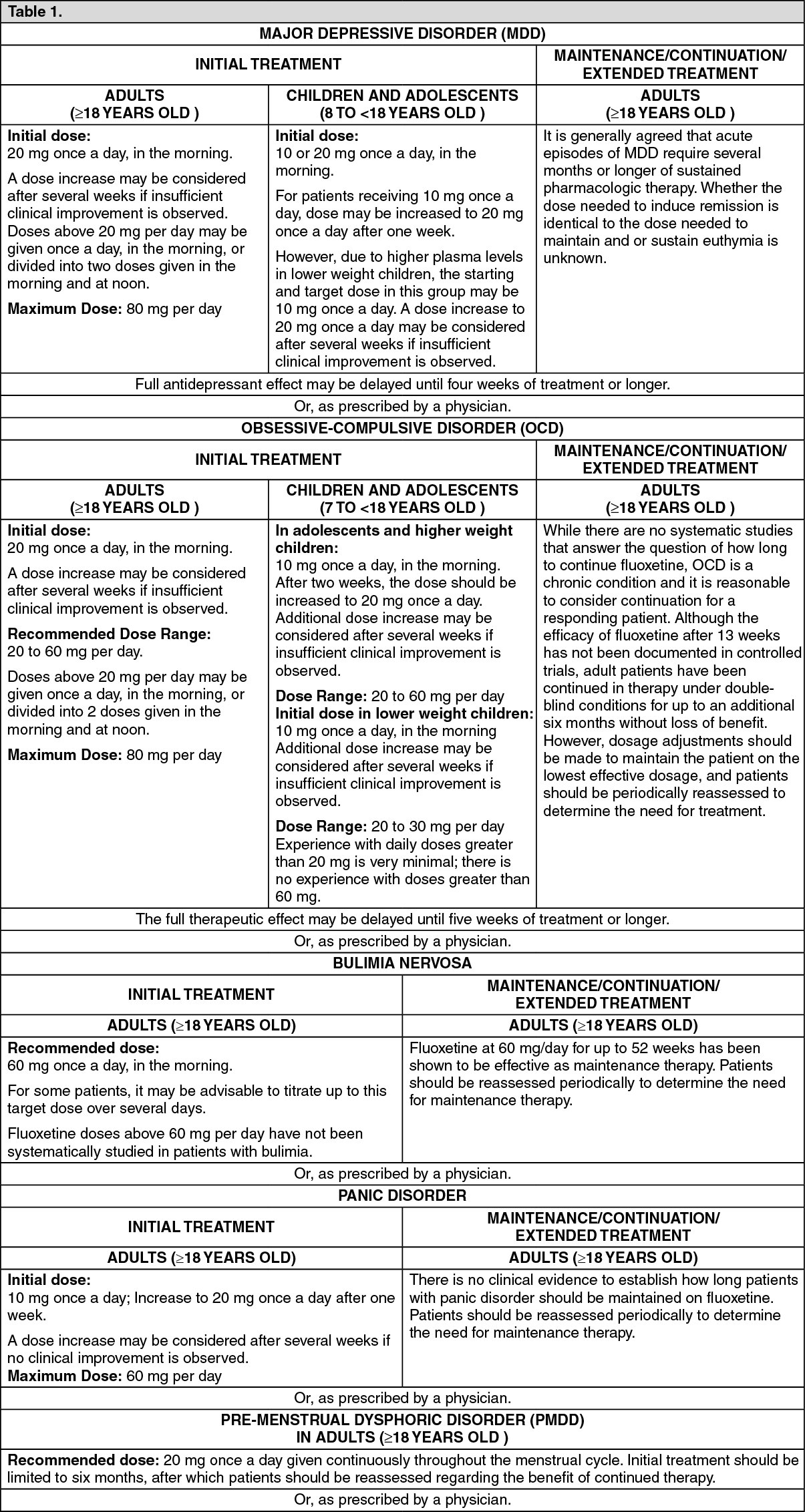 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image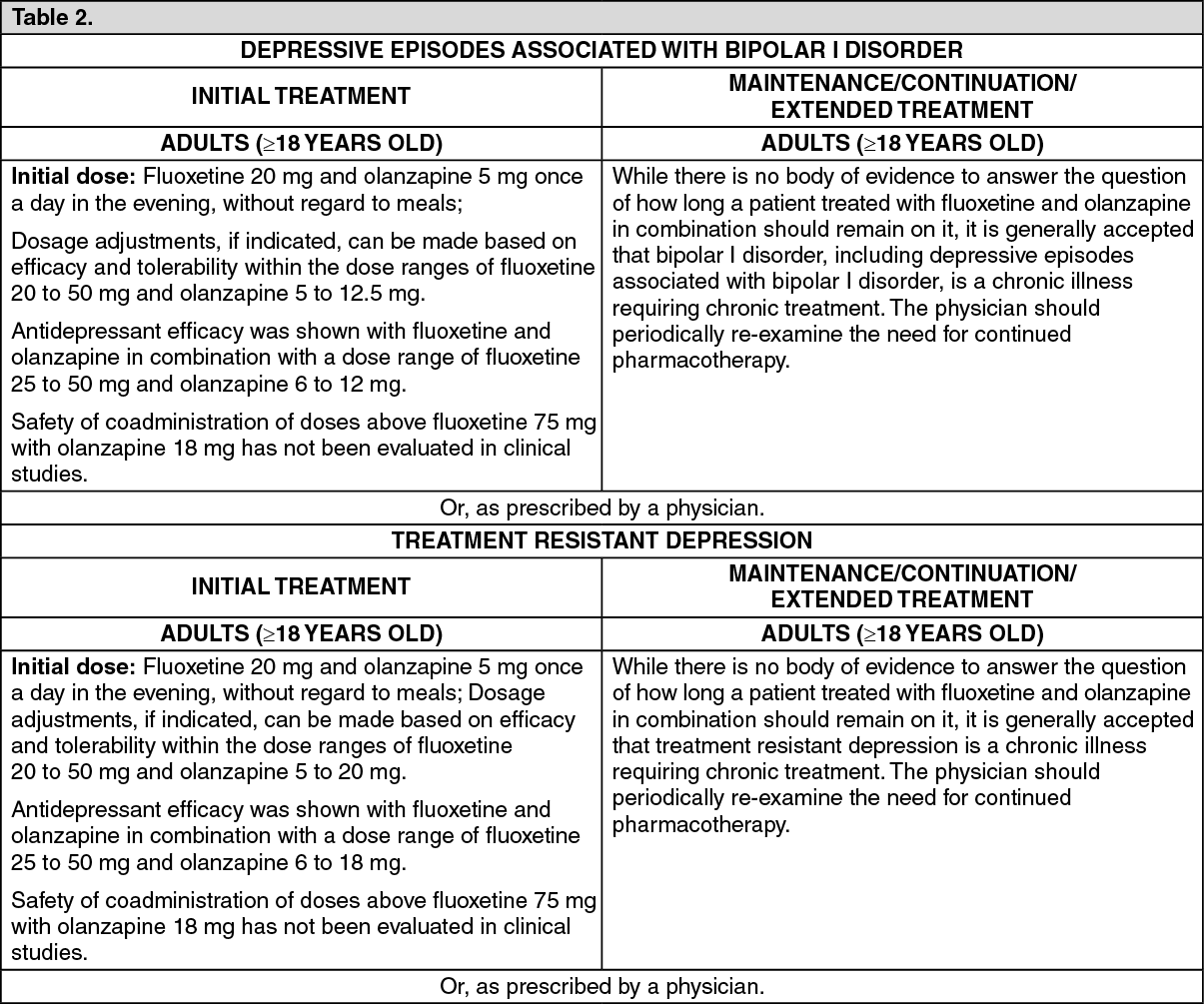 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out