Each vial contains: Omeprazole (as sodium), BP 40 mg.
Omeprazole Sodium (OMEE) 40 mg Lyophilized Powder for Injection is a white or off white lyophilized powder in 10 mL USP Type I Clear Glass Vial.
Pharmacology: Pharmacodynamics: Mechanism of Action: Omeprazole, a racemic mixture of two enantiomers reduces gastric acid secretion through a highly targeted mechanism of action. It is a specific inhibitor of the acid pump in the parietal cell. It is rapidly acting and provides control through reversible inhibition of gastric acid secretion with once daily dosing.
Omeprazole is a weak base and is concentrated and converted to the active form in the highly acidic environment of the intracellular canaliculi within the parietal cell, where it inhibits the enzyme H+, K+-ATPase - the acid pump. This effect on the final step of the gastric acid formation process is dose-dependent and provides for highly effective inhibition of both basal acid secretion and stimulated acid secretion, irrespective of stimulus.
Pharmacodynamic effects: All pharmacodynamics effects observed can be explained by the effect of omeprazole on acid secretion.
Effect on gastric acid secretion: Intravenous omeprazole produces a dose dependent inhibition of gastric acid secretion in humans. In order to immediately achieve a similar reduction of intragastric acidity as after repeated dosing with 20 mg orally, a first dose of 40 mg intravenously is recommended. This results in an immediate decrease in intragastric acidity and a mean decrease over 24 hours of approximately 90% for both IV injection and IV infusion. The inhibition of acid secretion is related to the area under the plasma concentration-time curve (AUC) of omeprazole and not to the actual plasma concentration at a given time. No tachyphylaxis has been observed during treatment with omeprazole.
Effect on H. pylori: H. pylori is associated with peptic ulcer disease, including duodenal and gastric ulcer disease. H. pylori is a major factor in the development of gastritis. H. pylori together with gastric acid are major factors in the development of peptic ulcer disease. H. pylori is a major factor in the development of atrophic gastritis which is associated with an increased risk of developing gastric cancer. Eradication of H. pylori with omeprazole and antimicrobials is associated with high rates of healing and long-term remission of peptic ulcers.
Other effects related to acid inhibition: During long-term treatment gastric glandular cysts have been reported in a somewhat increased frequency. These changes area physiological consequence of pronounced inhibition of acid secretion, are benign and appear to be reversible.
Decreased gastric acidity due to any means including proton pump inhibitors, increases gastric counts of bacteria normally present in the gastrointestinal tract. Treatment with acid-reducing drugs may lead to slightly increased risk of gastrointestinal infections such as Salmonella and Campylobacter. During treatment with antisecretory drugs serum gastrin increases in response to the decreased acid secretion. Also, CgA increases due to decreased gastric acidity. The increased CgA level may interfere with investigations for neuroendocrine tumours. Available published evidence suggests that proton pump inhibitor treatment should be discontinued between 5 days and 2 weeks prior to CgA measurement. This is to allow CgA levels that might be spuriously elevated following PPI treatment to return to reference range.
Pharmacokinetics: Distribution: The apparent volume of distribution in healthy subjects is approximately 0.3 l/kg body weight. Omeprazole is 97% plasma protein bound.
Metabolism: Omeprazole is completely metabolised by the cytochrome P450 system (CYP). The major part of its metabolism is dependent on the polymorphically expressed CYP2C19, responsible for the formation of hydroxyomeprazole, the major metabolite in plasma. The remaining part is dependent on another specific isoform, CYP3A4, responsible for the formation of omeprazole sulphone. As a consequence of high affinity of omeprazole to CYP2C19, there is a potential for competitive inhibition and metabolic drug-drug interactions with other substrates for CYP2C19. However, due to low affinity to CYP3A4, omeprazole has no potential to inhibit the metabolism of other CYP3A4 substrates. In addition, omeprazole lacks an inhibitory effect on the main CYP enzymes.
Approximately 3% of the Caucasian population and 15-20% of Asian populations lack a functional CYP2C19 enzyme and are called poor metabolisers. In such individuals the metabolism of omeprazole is probably mainly catalysed by CYP3A4. After repeated once-daily administration of 20 mg omeprazole, the mean AUC was 5 to 10 times higher in poor metabolisers than in subjects having a functional CYP2C19 enzyme (extensive metabolisers). Mean peak plasma concentrations were also higher, by 3 to 5 times. These findings have no implications for the posology of omeprazole.
Excretion: Total plasma clearance is about 30-40 l/h after a single dose. The plasma elimination half-life of omeprazole is usually shorter than one hour both after single and repeated once-daily dosing. Omeprazole is completely eliminated from plasma between doses. Almost 80% of a dose of omeprazole is excreted as metabolites in the urine, the remainder in the faeces, primarily originating from bile secretion.
Linearity/non-linearity: The AUC of omeprazole increases with repeated administration due to a decrease of systemic clearance probably caused by an inhibition of the CYP2C19 enzyme by omeprazole and/or its metabolites (e.g. the sulphone). No metabolite has been found to have any effect on gastric acid secretion.
Special populations: Impaired hepatic function: The metabolism of omeprazole in patients with liver dysfunction is impaired, resulting in an increased AUC. Omeprazole has not shown any tendency to accumulate with once-daily dosing.
Impaired renal function: The pharmacokinetics of omeprazole, including systemic bioavailability and elimination rate, are unchanged in patients with reduced renal function.
Elderly: The metabolism rate of omeprazole is somewhat reduced in elderly subjects (75-79 years of age).
Omeprazole sodium Powder for Injection is use for Duodenal ulcer, gastric ulcer and reflux oesophagitis and Zollinger-Ellison syndrome.
Posology: Alternative to oral therapy: In patients where the use of oral medicinal products is inappropriate, Omeprazole IV 40 mg once daily is recommended. In patients with Zollinger-Ellison Syndrome the recommended initial dose of Omeprazole given intravenously is 60 mg daily. Higher daily doses may be required and the dose should be adjusted individually. When doses exceed 60 mg daily, the dose should be divided and given twice daily. Omeprazole is to be administered in an intravenous infusion for 20-30 minutes.
Special populations: Impaired renal function: Dose adjustment is not needed in patients with impaired renal function.
Impaired hepatic function: In patients with impaired hepatic function a daily dose of 10-20 mg may be sufficient.
Elderly (>65 years old): Dose adjustment is not needed in the elderly.
Paediatric patients: There is limited experience with Omeprazole for intravenous use in children.
Method of administration: Omeprazole for intravenous is to be administered in an intravenous infusion for 20-30 minutes. After reconstitution the solution is colourless, clear, practically free from visible particles.
There is limited information available on the effects of overdoses of omeprazole in humans. In the literature, doses of up to 560 mg have been described, and occasional reports have been received when single oral doses have reached up to 2,400 mg omeprazole (120 times the usual recommended clinical dose). Nausea, vomiting, dizziness, abdominal pain, diarrhoea and headache have been reported. Also apathy, depression and confusion have been described in single cases.
The symptoms described in connection to omeprazole overdose have been transient, and no serious outcome has been reported. The rate of elimination was unchanged (first order kinetics) with increased doses. Treatment, if needed, is symptomatic.
Intravenous doses of up to 270 mg one single day and up to 650 mg over a three-day period have been given in clinical trials without any dose-related adverse reactions.
Hypersensitivity to omeprazole, substituted benzimidazoles or any of the excipients. Omeprazole like other Proton Pump Inhibitors should not be used concomitantly with nelfinavir.
In the presence of any alarm symptoms (e.g, significant unintentional weight loss, recurrent vomiting, dysphagia, haematemesis or melena) and when gastric ulcer is suspected or present, malignancy should be excluded, as treatment may alleviate symptoms and delay diagnosis.
Co-administration of atazanavir with proton pump inhibitors is not recommended. If the combination of atazanavir with a proton pump inhibitor is judged unavoidable, close clinical monitoring (e.g virus load) is recommended in combination with an increase in the dose of atazanavir to 400 mg with 100 mg of ritonavir; omeprazole 20 mg should not be exceeded.
Omeprazole, as all acid-blocking medicinal products, may reduce the absorption of vitamin B12 (cyanocobalamin) due to hypo- or achlorhydria. This should be considered in patients with reduced body stores or risk factors for reduced vitamin B12 absorption on long-term therapy.
Omeprazole is a CYP2C19 inhibitor. When starting or ending treatment with omeprazole, the potential for interactions with medicinal products metabolised through CYP2C19 should be considered. An interaction is observed between clopidogrel and omeprazole. The clinical relevance of this interaction is uncertain. As a precaution, concomitant use of omeprazole and clopidogrel should be discouraged.
Treatment with proton pump inhibitors may lead to slightly increased risk of gastrointestinal infections such as Salmonella and Campylobacter.
Severe hypomagnesaemia has been reported in patients treated with proton pump inhibitors like omeprazole for at least three months, and in most cases for a year. Serious manifestations of hypomagnesaemia such as fatigue, tetany, delirium, convulsions, dizziness and ventricular arrhythmia can occur but they may begin insidiously and be overlooked. In most affected patients, hypomagnesaemia improved after magnesium replacement and discontinuation of the proton pump inhibitor.
For patients expected to be on prolonged treatment or who take proton pump inhibitors with digoxin or medicinal products that may cause hypomagnesaemia (e.g., diuretics), health care professionals should consider measuring magnesium levels before starting proton pump inhibitor treatment and periodically during treatment.
Proton pump inhibitors, especially if used in high doses and over long durations (>1 year), may modestly increase the risk of hip, wrist and spine fracture, predominantly in the elderly or in presence of other recognised risk factors. Observational studies suggest that proton pump inhibitors may increase the overall risk of fracture by 10-40%. Some of this increase may be due to other risk factors. Patients at risk of osteoporosis should receive care according to current clinical guidelines and they should have an adequate intake of vitamin D and calcium.
Subacute cutaneous lupus erythematosus (SCLE): Proton pump inhibitors are associated with very infrequent cases of SCLE. If lesions occur, especially in sun-exposed areas of the skin, and if accompanied by arthralgia, the patient should seek medical help promptly and the health care professional should consider stopping omeprazole for intravenous. SCLE after previous treatment with a proton pump inhibitor may increase the risk of SCLE with other proton pump inhibitors.
Interference with laboratory tests: Increased Chromogranin A (CgA) level may interfere with investigations for neuroendocrine tumours. To avoid this interference, omeprazole for intravenous treatment should be stopped for at least 5 days before CgA measurements. If CgA and gastrin levels have not returned to reference range after initial measurement, measurements should be repeated 14 days after cessation of proton pump inhibitor treatment. As in all long-term treatments, especially when exceeding a treatment period of 1 year, patients should be kept under regular surveillance.
Pregnancy: Result from three epidemiological studies (more than 1,000 exposed outcomes) indicate no adverse events of omeprazole on pregnancy or on the health of the foetus/newborn child, Omeprazole can be used during pregnancy.
Lactation: Omeprazole is excreted in breast milk but is not likely to influence the child when therapeutic doses are used.
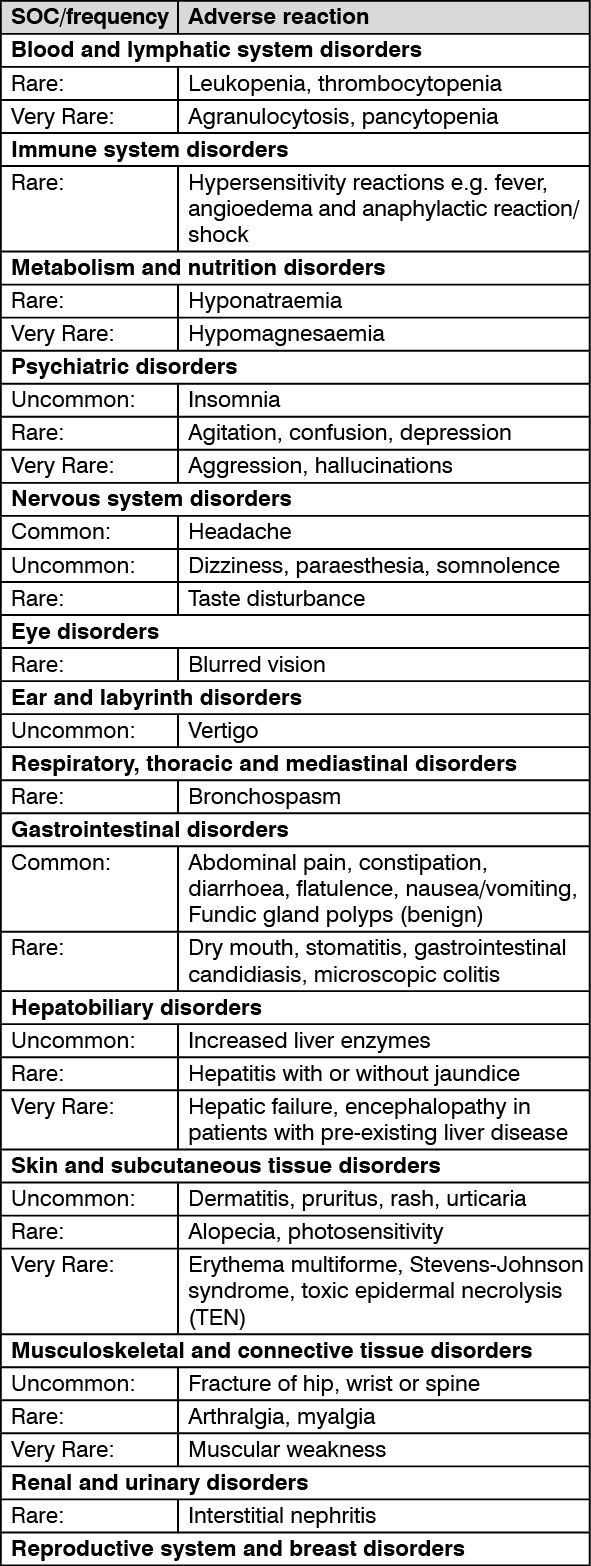
Frequency categories are defined according to the following convention: Very common (≥1/10), Common (≥1/100 to <1/10), Uncommon (≥1/1,000 to <1/100), Rare (≥1/10,000 to <1/1,000), Very rare (<1/10,000), Not known (cannot be estimated from the available data). (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Irreversible visual impairment has been reported in isolated cases of critically ill patients who have received omeprazole intravenous injection, especially at high doses, but no causal relationship has been established.
Effects of omeprazole on the pharmacokinetics of other active substances: Active Substances with PH dependent absorption: The decreased intragastric acidity during treatment with omeprazole might increase or decrease the absorption of active substances with a gastric pH dependent absorption.
Nelfinavir, atazanavir: The plasma levels of nelfinavir and atazanavir are decreased in case of co-administration with omeprazole. Concomitant administration of omeprazole with nelfinavir is contraindicated.
Co-administration of omeprazole (40 mg once daily) reduced mean nelvinavir exposure by ca. 40% and the mean exposure of the pharmacologically active metabolite M8 was reduced by ca. 75-90%. The interaction may also involve CYP2C19 inhibition.
Concomitant administration of omeprazole with atazanavir is not recommended. Concomitant administration of omeprazole (40 mg once daily) and atazanavir 300 mg/ritonavir 100 mg to healthy volunteers resulted in a 75% decrease of the atazanavir exposure. Increasing the atazanavir dose to 400 mg did not compensate for the impact of omeprazole on atazanavir exposure. The co-administration of omeprazole (20 mg once daily) with atazanavir 400 mg/ritonavir 100 mg to healthy volunteers resulted in a decrease of approximately 30% in the atazanavir exposure as compared to atazanavir 300 mg/ritonavir 100 mg once daily.
Digoxin: Concomitant treatment with omeprazole (20 mg daily) and digoxin in healthy subjects increased the bioavailability of digoxin by 10%. Digoxin toxicity has been rarely reported. However, caution should be exercised when omeprazole is given at high doses in elderly patients. Therapeutic drug monitoring of digoxin should then be reinforced.
Clopidogrel: In a crossover clinical study, clopidogrel (300 mg loading dose followed by 75 mg/day) alone and with omeprazole (80 mg at the same time as clopidogrel) were administered for 5 days. The exposure to the active metabolite of clopidogrel was decreased by 46% (Day 1) and 42% (Day 5) when clopidogrel and omeprazole were administered together. Mean inhibition of platelet aggregation (IPA) was diminished by 47% (24 hours) and 30% (Day 5) when clopidogrel and omeprazole were administered together. In another study it was shown that administering clopidogrel and omeprazole at different times did not prevent their interaction that is likely to be driven by the inhibitory effect of omeprazole on CYP2C19. Inconsistent data on the clinical implications of this PK/PD interaction in terms of major cardiovascular events have been reported from observational and clinical studies.
Other active substances: The absorption of posaconazole, erlotinib, ketoconazole and itraconazole is significantly reduced and thus clinical efficacy may be impaired. For posaconazole and erlotinib concomitant used should be avoided.
Active substances metabolised by CYP2C19: Omeprazole is a moderate inhibitor of CYP2C19, the major omeprazole metabolising enzyme. Thus, the metabolism of concomitant active substances also metabolised by CYP2C19, may be decreased and the systemic exposure to these substances increased. Examples of such drugs are R-warfarin and other vitamin K antagonists, cilostazol, diazepam and phenytoin.
Cilostazol: Omeprazole, given in doses of 40 mg to healthy subjects in a cross-over study, increased Cmax and AUC for cilostazol by 18% and 26% respectively, and one of its active metabolites by 29% and 69% respectively.
Phenytoin: Monitoring phenytoin plasma concentration is recommended during the first two weeks after initiating omeprazole treatment and, if a phenytoin dose adjustment is made, monitoring and a further dose adjustment should occur upon ending omeprazole treatment.
Unknown mechanism: Saquinavir: Concomitant administration of omeprazole with saquinavir/ritonavir resulted in increased plasma levels up to approximately 70% for saquinavir associated with good tolerability in HIV-infected patients.
Tacrolimus: Concomitant administration of omeprazole has been reported to increase the serum levels of tacrolimus. A reinforced monitoring of tacrolimus concentrations as well as renal function (creatinine clearance) should be performed, and dosage of tacrolimus adjusted if needed.
Effects of other active substances on the pharmacokinetics of omeprazole: Inhibitors of CYP2C19 and/or CYP3A4: Since omeprazole is metabolised by CYP2C19 and CYP3A4, active substances known to inhibit CYP2C19 or CYP3A4 (such as clarithromycin and voriconazole) may lead to increased omeprazole serum levels by decreasing omeprazole's rate of metabolism. Concomitant voriconazole treatment resulted in more than doubling of the omeprazole exposure. As high doses of omeprazole have been well-tolerated adjustment of the omeprazole dose is not generally required. However, dose adjustment should be considered in patients with severe hepatic impairment and if long-term treatment is indicated.
Inducers of CYP2C19 and/or CYP3A4: Active substances known to induce CYP2C19 or CYP3A4 or both (such as rifampicin and St John's wort) may lead to decreased omeprazole serum levels by increasing omeprazole's rate of metabolism.
Direction for Reconstitution: Dissolve the powder with Sterile Water for Injection: 1. With a Syringe draw 10 mL of solvent hem the ampoule.
2. Slowly add approximately 5 mL of the solvent into the vial with the powder.
3. Withdraw as much air as possible from the vial back into the syringe in order to reduce positive pressure. This will make it easier to add the remaining solvent.
4. Add the remaining solvent into the vial; make sure the syringe is empty.
5. Rotate and shake the vial to endure adequate mixing of omeprazole and solvent.
6. Reconstituted I.V. Solution shall be kept below 25°C and shall be used within 4 hours after preparation.
Store at temperatures not exceeding 30°C.
A02BC01 - omeprazole ; Belongs to the class of proton pump inhibitors. Used in the treatment of peptic ulcer and gastro-oesophageal reflux disease (GERD).
Omee lyo powd for inj 40 mg
(vial + 10 mL amp diluent) 10 × 1's; (vial + 10 mL amp diluent) 1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out