Direction for Reconstitution: Tap the bottle until all the powders flows freely. Add water up to the vertical circular mark and shake vigorously until the powder is evenly suspended. Refrigerate the suspension after reconstitution and use within 7 days. Do not freeze.
Shake the bottle well before each dose.
312.5 mg/5 mL: Children : The usual recommended daily dosage is 25 mg/kg/day in divided doses every eight hours. Under 1 year: 25 mg/kg/day a 7.5 kg child would require 2 mL of Co-Amoxiclav 156.25 mg/5mL Suspension three times a day.
1-6 years (10-18 kg): 5 mL of Co-Amoxiclav 156.25mg/5mL Suspension three times a day.
Over 6 years (18-40 kg): 5 mL of Co-Amoxiclav 312.5mg/5mL Suspension three times a day.
Or as prescribed by the physician.
Renal impairment: Dose adjustments are based on the maximum recommended level of amoxicillin.
No adjustment in dose is required in patients with creatinine clearance (CrCl) greater than 30 ml/min.
Children <40 kg: CrCl: 10-30 ml/min-15 mg/3.75 mg/kg twice daily (maximum 500 mg/125 mg twice daily).
CrCl: 10-30 ml/min-15 mg/3.75 mg/kg as a single daily dose (maximum 500 mg/125 mg).
Hemodialysis: 15 mg/3.75 mg/kg per day once daily. Prior to haemodialysis 15 mg/3.75 mg/kg. In order to restore circulating drug levels, 15mg/3.75 mg per kg should be administered after haemodialysis.
Hepatic impairment: Dose with caution and monitor hepatic function at regular intervals.
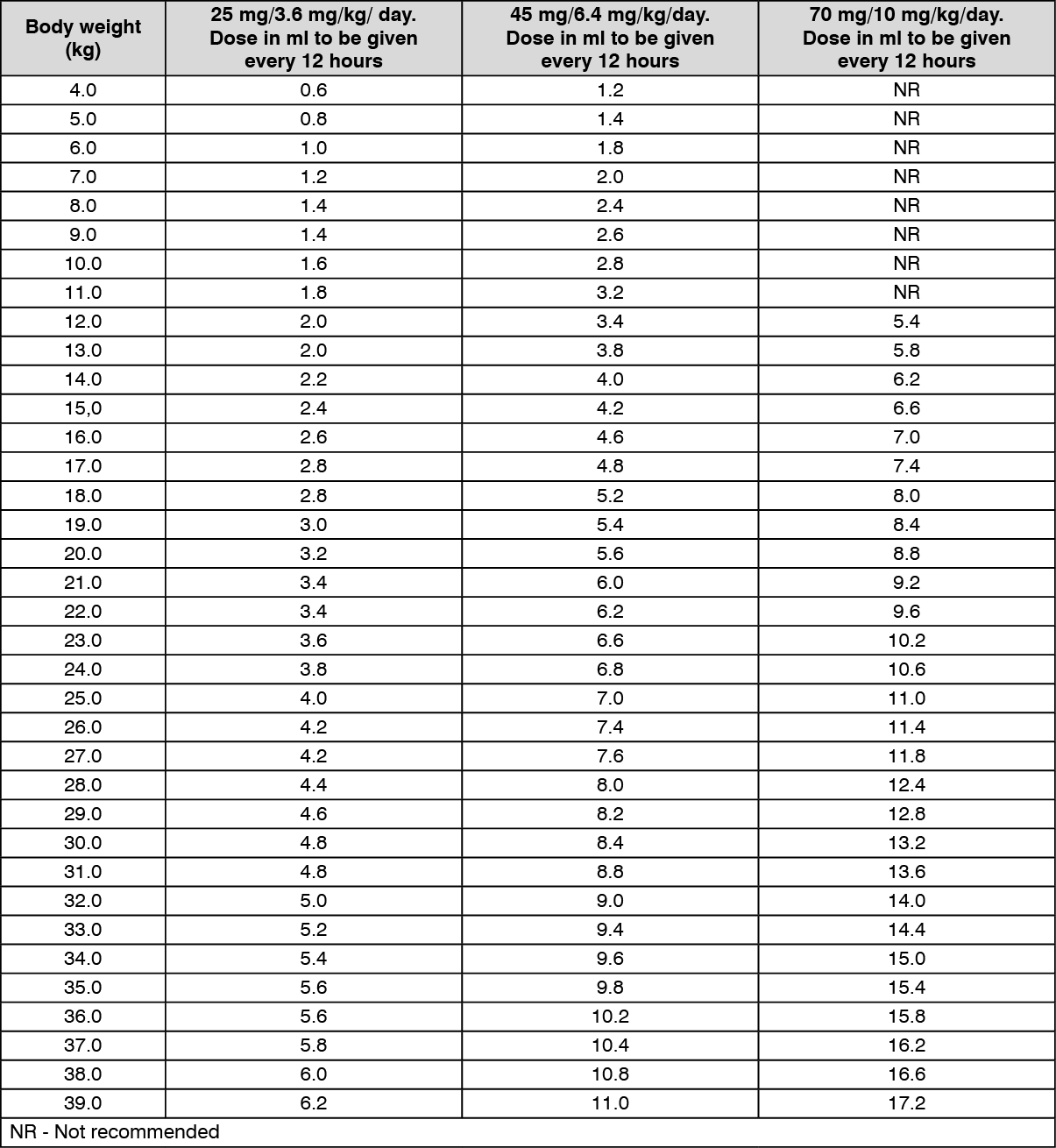
457 mg/5 mL: For children <40 kg, this formulation of amoxicillin/clavulanic provides a maximum daily dose of 1000-2800 mg amoxicillin/143-400 mg clavulanic acid, when administered as recommended as follows. If it is considered that a higher daily dose of amoxicillin is required, it is recommended that another preparation of amoxicillin/clavulanic is selected in order to avoid administration of unnecessarily high daily doses of clavulanic acid.
Adults and children ≥40 kg should be treated with the adult formulations of amoxicillin/clavulanic.
Children <40 kg: Lower dose: 25 mg/3.6 mg/kg/day to 45 mg/6.4 mg/kg/day given as two divided doses; Higher dose: 45 mg/6.4 mg/kg/day to 70 mg/10 mg/kg/day given as two divided doses may be considered for some infections (such as otitis media, sinusitis and lower respiratory tract infections). (See Table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The duration of therapy should be determined by the response of the patient. Some infections (e.g. osteomyelitis) require longer periods of treatment. Treatment should not be extended beyond 14 days without review.
There are no clinical data for amoxicillin/clavulanic 7:1 formulations for patients under 2 months of age. Dosing recommendations in this population therefore cannot be made.
Children aged 6 years and below should preferably be treated with amoxicillin/clavulanic suspension.
Elderly: No dose adjustment is considered necessary. Elderly patients should be treated with adult formulations.
Renal impairment: No dose adjustment is required in patients with creatinine clearance (CrCl) greater than 30 ml/min.
In patients with creatinine clearance less than 30 ml/min, the use of amoxicillin/clavulanic presentations with an amoxicillin to clavulanic acid ratio of 7:1 is not recommended, as no recommendations for dose adjustments are available.
Hepatic impairment: Dose with caution and monitor hepatic function at regular interval.
Method of administration: For oral use.
Administer at the start of a meal to minimise potential gastrointestinal intolerance and optimise absorption of amoxicillin/clavulanic acid.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
