


 Sign Out
Sign Out

Severe cutaneous reactions: Severe cutaneous reactions have been reported with alpelisib (Pivikto). In the Phase III clinical study, Stevens-Johnson syndrome (SJS) and erythema multiforme (EM) were reported in 1 (0.4%) and 3 (1.1%) patients, respectively. Drug reaction with eosinophilia and systemic symptoms (DRESS) has been reported in the post marketing setting (see ADVERSE REACTIONS).
Alpelisib (Pivikto) treatment should not be initiated in patients with history of severe cutaneous reactions.
Patients should be advised of the signs and symptoms of severe cutaneous reactions (e.g. a prodrome of fever, flu-like symptoms, mucosal lesions or progressive skin rash). If signs or symptoms of severe cutaneous reactions are present, alpelisib (Pivikto) should be interrupted until the etiology of the reaction has been determined. A consultation with a dermatologist is recommended. If a severe cutaneous reaction is confirmed, alpelisib (Pivikto) should be permanently discontinued. Alpelisib (Pivikto) should not be reintroduced in patients who have experienced previous severe cutaneous reactions. If a severe cutaneous reaction is not confirmed, alpelisib (Pivikto) may require treatment interruption, dose reduction, or treatment discontinuation as described in Table 5 Dose modification and management for rash (see DOSAGE & ADMINISTRATION).
Hyperglycemia: Severe hyperglycemia, in some cases associated with hyperglycemic hyperosmolar nonketotic syndrome (HHNKS) or ketoacidosis, has been observed in patients treated with alpelisib (Pivikto). Some cases of ketoacidosis with fatal outcome have been reported in the post marketing setting.
Hyperglycemia was reported in 64.8% of patients treated with alpelisib (Pivikto) in the phase III clinical study. Grade 2 (FPG 160 to 250 mg/dL), 3 (FPG >250 to 500 mg/dL) or 4 (FPG > 500 mg/dL) hyperglycemia were reported in 15.8%, 33.1% and 3.9% of patients, respectively, in phase III clinical study.
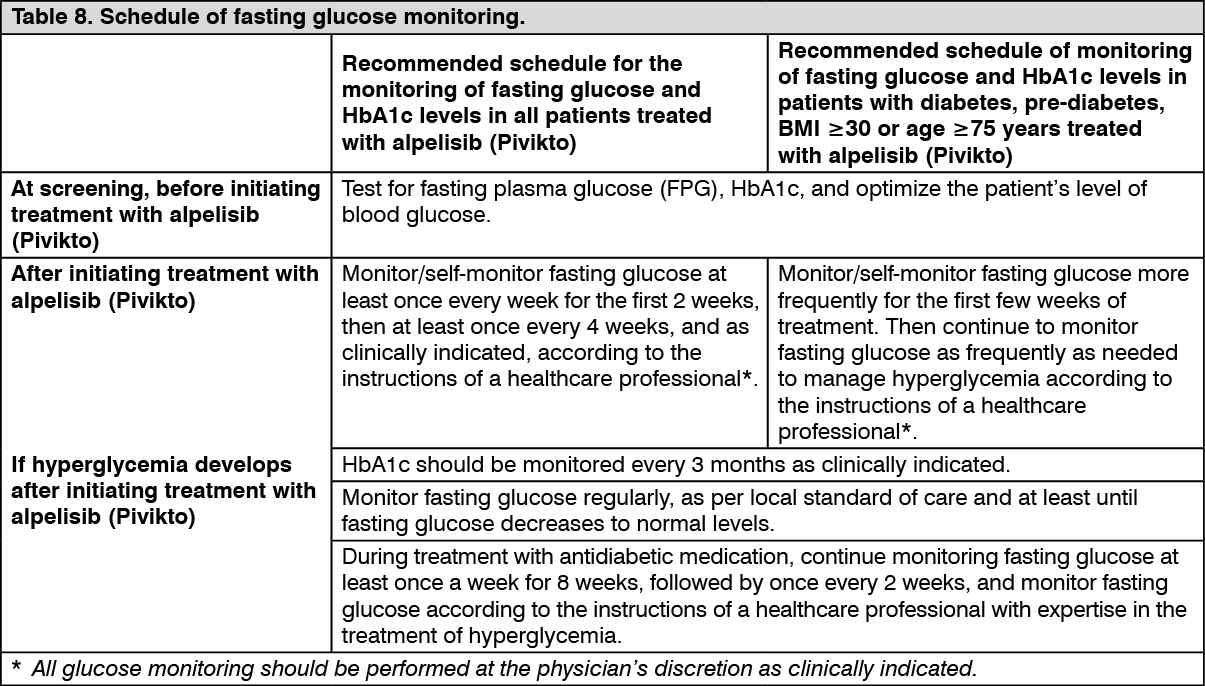
In the phase III clinical study, patients with a history of diabetes mellitus intensified anti-diabetic medication(s) while on treatment with alpelisib (Pivikto); therefore, these patients require monitoring and possibly intensified anti-diabetic treatment. Patients with poor glycemic control may be at a higher risk of developing severe hyperglycemia and associated complications. Patients with risk factors for hyperglycemia such as obesity (BMI ≥30), elevated FPG or HbA1c at or above the upper limit of normal, or age ≥75 are at a higher risk of developing severe hyperglycemia. Schedule for monitoring fasting glucose is presented in Table 8.
Patients should be advised of the signs and symptoms of hyperglycemia (e.g. excessive thirst, urinating more often than usual or higher amount of urine than usual, increased appetite with weight loss). (See Table 8.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn patients with hyperglycemia, 163/187 (87.2%) were managed with anti-diabetic medication and 142/187 (75.9%) reported use of metformin as single agent or in combination with other anti-diabetic medication. The maximum dose of metformin recommended in phase III clinical study was 2,000 mg per day.
In patients with hyperglycemia of at least Grade 2 (FPG 160 to 250 mg/dL), median time to improvement by at least 1 Grade of the first event was 8 days (95% CI of 8 to 10 days). In all patients with elevated FPG, who continued fulvestrant treatment after discontinuing alpelisib (Pivikto), all FPG levels returned to baseline (normal).
Based on the severity of the hyperglycemia, alpelisib (Pivikto) may require dose interruption, reduction, or discontinuation as described in Table 4 Dose modification and management for hyperglycemia. (see DOSAGE & ADMINISTRATION).
Pneumonitis: Pneumonitis including serious cases of pneumonitis/acute interstitial lung disease have been reported in alpelisib (Pivikto) treated patients in clinical studies. Patients should be advised to promptly report any new or worsening respiratory symptoms. In patients who have new or worsening respiratory symptoms or are suspected to have developed pneumonitis, alpelisib (Pivikto) treatment should be interrupted immediately and the patient should be evaluated for pneumonitis. A diagnosis of non-infectious pneumonitis should be considered in patients presenting with non-specific respiratory signs and symptoms such as hypoxia, cough, dyspnea, or interstitial infiltrates on radiologic exams and in whom infectious, neoplastic, and other causes have been excluded by means of appropriate investigations. Alpelisib (Pivikto) should be permanently discontinued in all patients with confirmed pneumonitis.
Diarrhea or colitis: Severe diarrhea and clinical consequences, such as dehydration and acute kidney injury have been reported during treatment with alpelisib (Pivikto) in clinical studies(see Table 9 ADVERSE REACTIONS). In the phase III clinical study, Grade 2 and 3 diarrhea were reported in 18.3% and 6.7% of patients, respectively. There were no reported cases of Grade 4 diarrhea. Among patients with Grade 2 or 3 diarrhea, median time to onset was 46 days (range: 1 to 442 days).
Colitis has been reported in the post marketing setting in patients treated with alpelisib (Pivikto) (see ADVERSE REACTIONS).
In the phase III clinical study, dose reductions of alpelisib (Pivikto) were required in 6% of patients and 2.8% of patients permanently discontinued alpelisib (Pivikto) due to diarrhea.
Patients should be monitored for diarrhea and additional symptoms of colitis, such as abdominal pain and mucus or blood in stool. Based on the severity of the diarrhea or colitis, Alpelisib (Pivikto) may require dose interruption, reduction, or discontinuation as described in Table 6 (see DOSAGE & ADMINISTRATION).
Patients should be advised to notify the healthcare provider if diarrhea or additional symptoms of colitis occur while taking alpelisib (Pivikto). Patients should be managed according to local standard of care medical management, including electrolyte monitoring, administration of anti-emetics and antidiarrheal medications and/or fluid replacement and electrolyte supplements, as clinically indicated. In case of colitis, additional treatment, such as steroids, may be considered as clinically indicated.
Osteonecrosis of the jaw: Caution should be exercised when alpelisib (Pivikto) and bisphosphonates or denosumab are used either simultaneously or sequentially. Alpelisib (Pivikto) treatment should not be initiated in patients with ongoing osteonecrosis of the jaw from previous or concurrent treatment with bisphosphonates/denosumab. Patients should be advised to promptly report any new or worsening oral symptoms (such as dental mobility, pain or swelling, non-healing of mouth sores, or discharge) during treatment with alpelisib (Pivikto).
In patients who develop osteonecrosis of the jaw, standard medical management should be initiated.