


 Sign Out
Sign Out
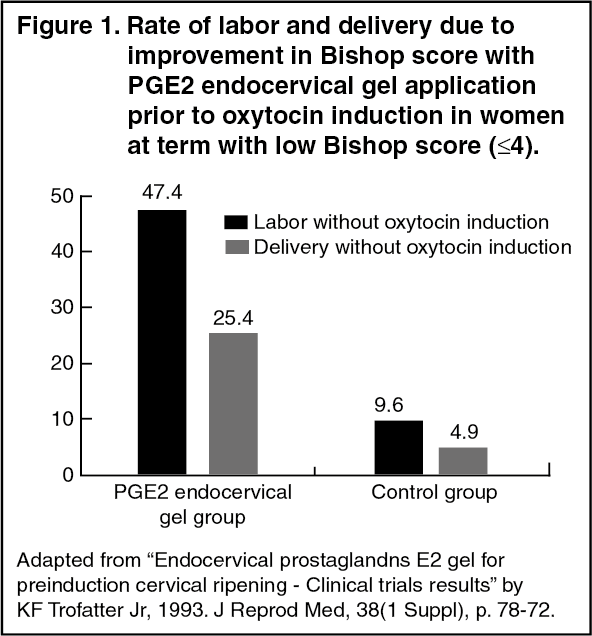
Clinical trials: Among all the routes of prostaglandin administration available for cervical ripening ad labor induction, endocervical PGE2 is a valuable option due to increased efficacy and low incidence of side effects associated with it.
Primigyn, an endocervical PGE2 gel, is used extensively for preinduction cervical ripening and labor induction. This is based on a repertoire of clinical trials which attest the significant efficacy and safety of endocervical PGE2 gel in cervical ripening and induction of labor. A randomized clinical trial evaluated the efficacy and safety of PGE2 endocervical gel (0.5 mg in 2-2.5 ml gel base) for preinduction cervical ripening prior to oxytocin induction. The study involved 538 women at term with low Bishop score (i.e., S4) who were treated with either PGE2 endocervical gel 12 hours prior to labor induction with oxytocin (PGE2 endocervical gel group) or with oxytocin induction alone (control group). During the 12- hour ripening period, patients in PGE2 endocervical group compared with control group achieved significant improvement in Bishop score which translated into high rate of labor (47.4% vs 9.6%, P < 0.001; figure 1). Deliveries without oxytocin occurred in 25.4% patients in the PGE2 endocervical gel group and in only 4.9% patients in the control group (figure 1). Endocervical application of PGE2 gel also reduced the time between induction, delivery and the duration of oxytocin administration. Equivalent maternal and fetal outcomes and incidence of complications denoted safety of PGE2 endocervical gel for cervical ripening of an unfavorable cervix. Similarly, another open randomized clinical trial yet again demonstrated that endocervical application of PGE2 gel in pregnant women at term with low Bishop score is significantly effective in cervical ripening and labor induction. The study women (n=100) were randomized into two groups: PGE2 endocervical gel group who were treated with PGE2 endocervical (0.5 mg in 2.5 ml gel) 12 hours before oxytocin labor induction, and control group who received oxytocin infusion alone. Notably, Bishop score progressed at least 3 points in 92% women in the PGE2 endocervical gel group whereas the mean Bishop score in the control group increased insignificantly. During the 12-hour ripening period before oxytocin induction, 32% women in the PGE2 endocervical gel group and 6% women in the control group delivered (figure 2). Of the remaining women who underwent oxytocin induction, the first induction attempt was successful in 64% women in the PGE2 endocervical gel group and 57% women in the control group (figure 2). Cesarean section rate was also lower in the former group compared with the latter (10% and 12%, respectively, figure 2). The safety ofpGE2 endocervical gel was reflected by no serious maternal or fetal side effects.
A multicentric prospective, randomized trial corroborated the aforementioned findings by showing a single application of PGE2 endocervical gel (0.5 mg in 2.5 ml gel) 12 hours prior to oxytocin induction in women at term with low Bishop score to achieve successful initial induction in 83% of patients compared to 58% success in non-primed controls (figure 3).
The researchers also noted that the induction delivery interval was shorter in the PGE2 endocervical gel group compared with the control group (median times 9.0 vs 11.3 hours. Additionally, the rate of cesarean section was lower in the former group than the latter (16% vs 21%, respectively).
It was concluded that the endocervical PGE2 gel application is an effective and well-tolerated method of cervical ripening prior to oxytocin induction in term pregnant women with unfavorable cervices.' The endocervical application of PGE2 gel has also been found to be more efficacious than PGE2 vaginal tablets. A randomized double blind study compared the efficacy and safety of endocervical PGE2 gel (0.5 mg of PGE2 in 3 g of the gel; PGE2 endocervical gel group) for preinduction cervical ripening with PGE2 vaginal tablets (2.0 mg tablet; PGE2 vaginal tablet group) and placebo treatment (placebo group) in at term, nulliparous women with low Bishop score. The overall success was defined as a progression in Bishop score of at least 3 points within 12 hours. While 55% women in PGE2 endocervical gel group achieved success, only 37% in PGE2 vaginal tablet group and 20% in the placebo group documented success(figure 4), Even in women with very unfavorable cervices (Bishop score 0-2), PGE2 endocervical gel maintained its superiority over its comparators ; the success rates were 75%, 15% and 0%, respectively, A very low incidence of side effects attested the safety of PGE2 endocervical gel. Similar comparisons between PGE2 endocervical gel and PGE2 vaginal gel have revealed the former formulation s to be more effective than the latter in achieving cervical ripeness. When compared with intravaginal misoprostol (PGEl) for labor induction, although the two methods are equally effective in achieving active labor and delivering within 24 hours, it is noteworthy that PGE2 endocervical gel is more safe due to lower incidence of uterine hyperstimulation and tachysystole. Overall, based on the tangible evidence it may be summated that endocervical application of PGE2 gel is an efficacious and well tolerated method to facilitate cervical ripening in pregnant women at term with unfavorable cervices for labor induction. (See Figures 1, 2, 3, and 4).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image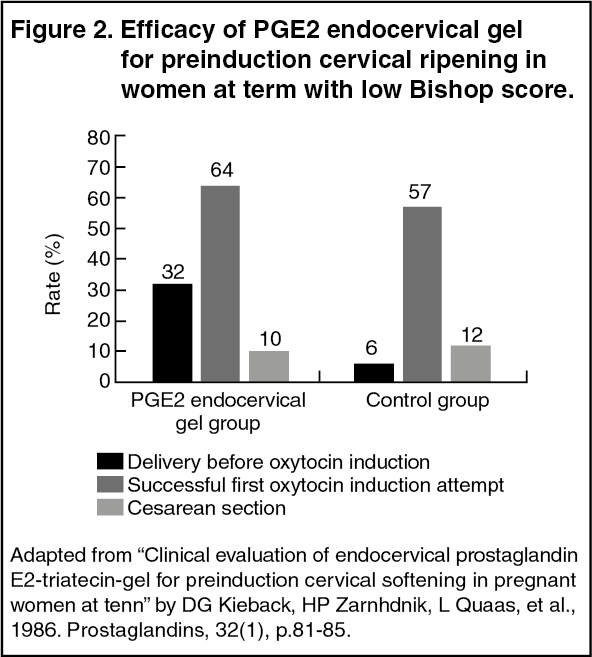 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image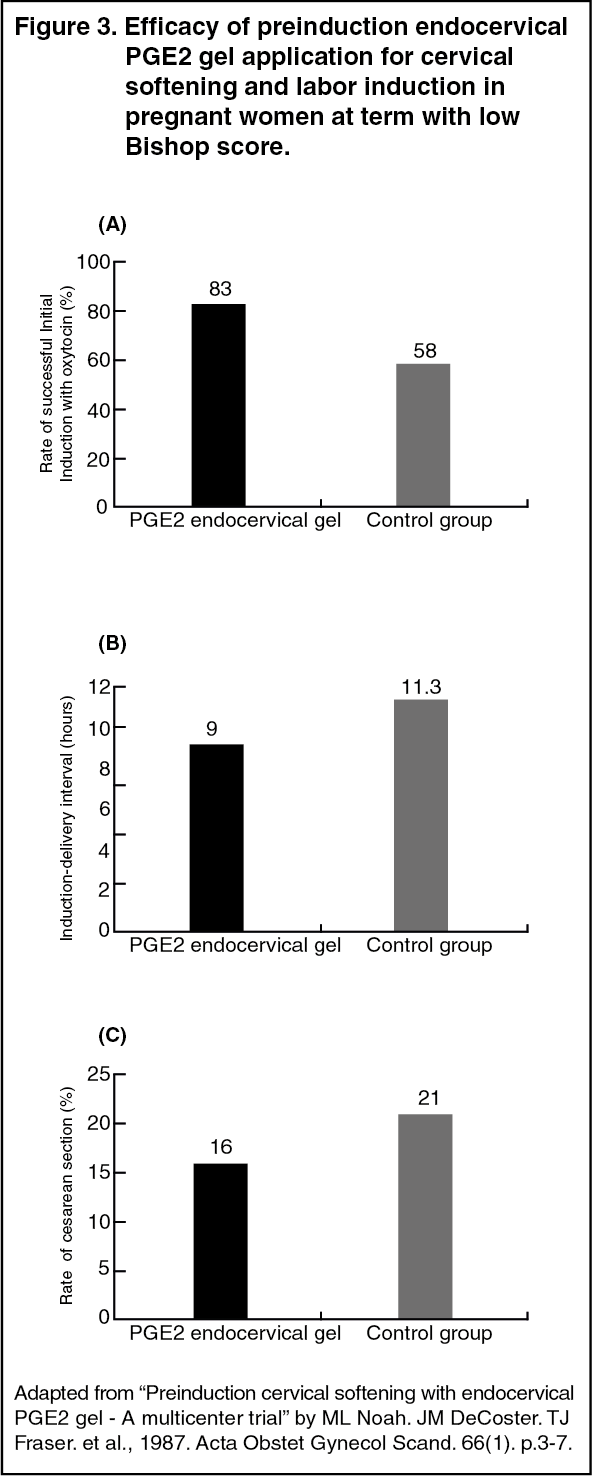 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image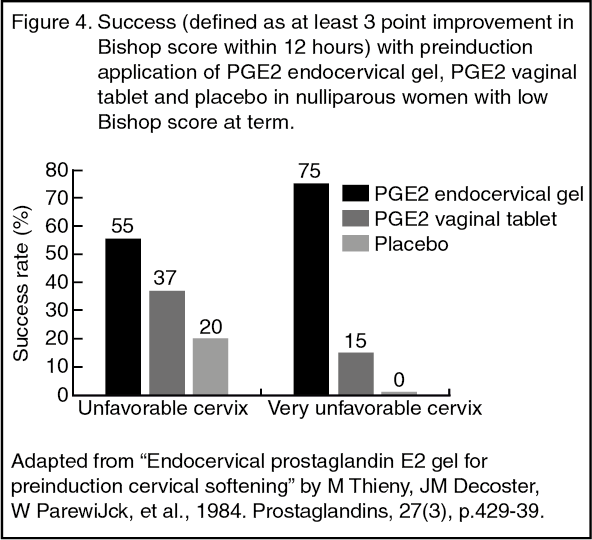 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePharmacokinetics: Absorption: Time taken to reach the maximum concentration (Tmax) 0.5 to 0.75 hours, maximum concentration (Cmax) 484 pg/mL.
Metabolism: Primigyn is rapidly metabolized in the cervical tissues by oxidative pathways.
Elimination: Half-life (t½) 2.5-5 minutes. The metabolic products are excreted by the kidneys in the urine.