Capsule: Most adverse effects reported with cefixime were similar to those reported with other oral cephalosporins and were usually mild and transient in nature.
Gastrointestinal (GI): Abdominal pain, anorexia, diarrhea, dry mouth, dyspepsia, flatulence, loose or frequent stools/stool changes, nausea, vomiting, pseudomembranous colitis, pruritus ani.
Dermatologic/Hypersensitivity Reactions: Anaphylactic/anaphylactoid reactions (including shock and fatalities), angioedema, arthralgia, drug fever, erythema multiforme, facial edema, pruritus, skin rashes, serum sickness-like reactions, Stevens-Johnson syndrome, toxic epidermal necrolysis, drug rash with eosinophilia and systemic symptoms (DRESS), urticaria.
Hepatic: Transient elevation of alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase, bilirubin, and lactate dehydrogenase (LDH); hepatitis, jaundice (cholestatic and/or hepatocellular).
Renal/Genitourinary: Transient elevations in blood urea nitrogen (BUN) and serum creatinine levels; acute renal failure including tubulointerstitial nephritis; dysuria, pyuria, genital pruritus, vaginitis, vaginal candidiasis.
Nervous System: Dizziness, headache, fatigue, insomnia, malaise, nervousness, seizures, somnolence.
Hematologic: Transient thrombocytopenia, thrombocytosis, leucopenia, leukocytosis, neutropenia, agranulocytosis, eosinophilia, and hypereosinophilia, immune hemolytic anemia; prolonged prothrombin time, prolonged partial thromboplastin time, decreased hemoglobin concentration and hematocrit.
Abnormal Laboratory Test: Hyperbilirubinemia.
Other Adverse Effects: Increased serum amylase concentrations; dyspnea, respiratory distress.
In addition to the adverse reactions listed previously which have been observed in patients treated with cefixime, the following adverse reactions and altered laboratory tests have been reported for cephalosporin-class antibiotics.
Allergic reactions, hypersensitivity reactions including chills, joint pain or inflammation, hypotension; renal dysfunction, toxic nephropathy, hepatic dysfunction including cholestasis; aplastic anemia, epistaxis or hemorrhage, thrombocythemia, granulocytosis, monocytosis, lymphocytopenia, basophilia, hypoprothrombinemia (with or without bleeding), menstrual irregularities, tenesmus, epigastric pain, glossitis, candidiasis (oral thrush), taste alteration, decreased salivation, heartburn, colitis, nightmares, vertigo, chest pain, pleural effusion, pulmonary infiltrate, cough and rhinitis, increased or decreased serum glucose concentration; superinfection.
Granules for oral suspension: The most common are hypersensitivity reactions, including skin rashes, urticaria, eosinophilia, fever, reactions resembling serum sickness, and anaphylaxis. There may be a positive response to the Coombs' test although haemolytic anaemia rarely occurs. Neutropenia and thrombocytopenia have occasionally been reported. Agranulocytosis has been associated rarely with some cephalosporins. Bleeding complications related to hypoprothrombinaemia and/or platelet dysfunction have occurred especially with cephalosporins and cephamycins having a methylthiotetrazole side-chain, including cefamandole, cefbuperazone, cefmenoxime, cefmetazole, cefonicid, cefoperazone, ceforanide, cefotetan, cefpiramide, and latamoxef. The presence of a methylthiadiazolethiol side-chain, as in cefazolin, or a methylthiotriazine ring, as in ceftriaxone, might also be associated with such bleeding disorders.


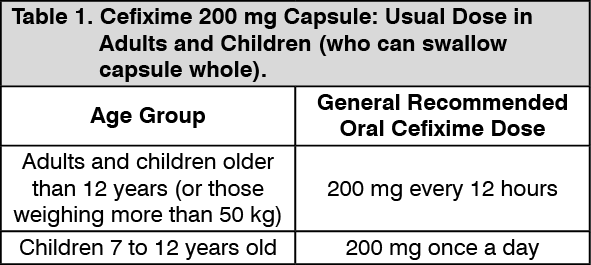 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image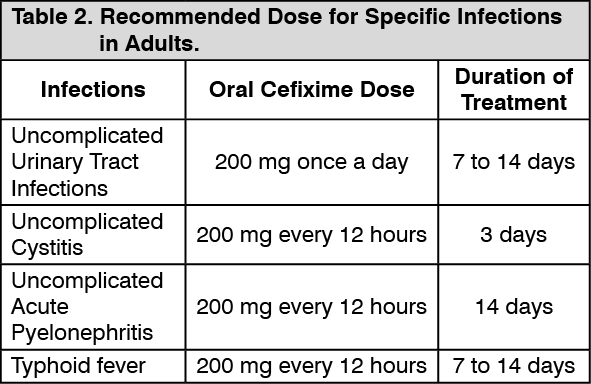 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
