Body as a Whole: Asthenia, infection, accidental injury, fatigue, viral infection, fever, malaise, face edema, allergy, generalized edema, chill, lassitude, alcohol intolerance, hangover effect, abscess, mucous membrane disorder, body odor, lump in neck.
Nervous System: Headache, dizziness, somnolence, ataxia, abnormal thinking, abnormal gait, incoordination, amnesia, hypoesthesia, dysesthesia, hyperesthesia, nystagmus, tremor, nervousness, dysarthria, depression, twitching, abnormal coordination, hostility, emotional lability, hyperkinesia, strange feelings, vertigo, paresthesia, decreased or absent reflexes, increased reflexes, anxiety, CNS tumors, abnormal dreaming, aphasia, intracranial hemorrhage, hypotonia, paresis, dystonia, hemiplegia, facial paralysis, stupor, cerebellar dysfunction, positive Babinski sign, decreased position sense, subdural hematoma, apathy, hallucination, agitation, paranoia, depersonalization, euphoria, feeling high, doped-up sensation, suicide attempt, psychosis, choreathetosis, orofacial dyskinesia, encephalopathy, nerve palsy, personality disorder, subdued temperament, apraxia, fine motor control disorder, meningismus, local myoclonus, hypokinesia, mania, neurosis, hysteria, antisocial reaction, migraine, confusion, insomnia, neuropathy, speech disorder, circumoral paresthesia, hypertonia, movement disorder, vestibular disorder.
Cardiovascular: Vasodilation, hypertension, hypotension, angina pectoris, peripheral vascular disorder, palpitation, tachycardia, bradycardia, murmur, atrial fibrillation, heart failure, thrombophlebitis, myocardial infarction, cerebrovascular accident, pulmonary thrombosis, ventricular extrasystoles, premature atrial contraction, pericardial rub, heart block, pulmonary embolus, pericardial effusion, pericarditis, syncope, chest pain, cardiovascular disorder, congestive heart failure, increased capillary fragility, phlebitis, varicose vein.
Gastrointestinal: Abdominal pain, diarrhea, dry mouth, constipation, nausea, vomiting, flatulence, dyspepsia, dental abnormalities, gingivitis, glossitis, gum hemorrhage, thirst, stomatitis, increased salivation, gastroenteritis, hemorrhoids, bloody stools, fecal incontinence, hepatomegaly, dysphagia, eructation, pancreatitis, peptic ulcer, colitis, blisters in mouth, tooth discolor, perleche, enlarged salivary gland, lip hemorrhage, esophagitis, hiatal hernia, hematemesis, proctitis, irritable bowel syndrome, rectal hemorrhage, esophageal spasm, oral moniliasis, gastritis, tooth disorder, abnormal stools, periodontal abscess, cholecystitis, cholelithiasis, duodenal ulcer, gamma glutamyl transpeptidase increased, intestinal obstruction, intestinal ulcer, melena, mouth ulceration, rectal disorder.
Metabolic and Nutritional: Peripheral edema, weight gain, weight loss, hyperglycemia, increased appetite, hyperlipidemia, hypercholesterolemia, anorexia, impotence, decreased libido, increased libido, ejaculation abnormal, hyperthyroid, hypothyroid, goiter, hypoestrogen, ovarian failure, epididymitis, swollen testicle, cushingoid appearance, diabetes mellitus, gout, hypoglycemia, alkaline phosphatase increased, diabetic ketoacidosis, lactic dehydrogenase increased.
Hematologic: Leukopenia, decreased WBC count, increased WBC count, purpura, anemia, thrombocytopenia, lymphadenopathy, lymphocytosis, non-Hodgkin's lymphoma, increased bleeding time, sepsis, ecchymosis, lymphoma-like reaction, prothrombin decreased.
Urogenital/Reproductive: Hematuria, dysuria, urination frequency, cystitis, abnormal blood urea nitrogen (BUN) value, urinary tract infection, urinary incontinence, vaginal moniliasis, breast pain, menstrual disorder, polyuria, urinary retention, cystitis, swollen penis, gynecomastia, nocturia, pyelonephritis, swollen scrotum, urinary urgency, urine abnormality.
Hepatic: Liver function tests abnormal.
Musculoskeletal: Back pain, myalgia, fracture, arthralgia, tendonitis, arthritis, joint stiffness, joint swelling, positive Romberg test, costochondritis, osteoporosis, bursitis, contracture, neck pain, pelvic pain, arthrosis, leg cramps, myasthenia, shin bone pain, joint disorder, tendon disorder.
Respiratory: Pharyngitis, coughing, bronchitis, respiratory infection, pneumonia, epistaxis, dyspnea, apnea, mucositis, aspiration pneumonia, hyperventilation, hiccup, laryngitis, nasal obstruction, snoring, bronchospasm, hypoventilation, lung edema, rhinitis, sinusitis, asthma, lung disorder, hemoptysis, voice alteration.
Skin and appendages: Rash, abrasion, pruritus, alopecia, eczema, dry skin, increased sweating, urticaria, hirsutism, seborrhea, cyst, herpes simplex, herpes zoster, skin discolor, skin papules, photosensitive reaction, leg ulcer, scalp seborrhea, psoriasis, desquamation, maceration, skin nodules, subcutaneous nodule, melanosis, skin necrosis, local swelling, cellulitis, skin ulcer, skin disorder, fungal dermatitis, furunculosis, vesiculobullous rash, acne, hair disorder, maculopapular rash, nail disorder, skin carcinoma, skin hypertrophy.
Special Senses: Amblyopia, conjunctivitis, diplopia, eyes dry, eye pain, visual field defect, photophobia, bilateral or unilateral ptosis, eye hemorrhage, eye twitching, hordeolum, retinal vein thrombosis, conjunctival hyperemia, diabetic retinopathy, fundi with microhemorrhage, abnormal vision, eye itching, abnormal accommodation, eye focusing problem, watery eyes, retinopathy, glaucoma, iritis, corneal disorders, lacrimal dysfunction, degenerative eye changes, blindness, retinal degeneration, miosis, chorioretinitis, strabismus, otitis media, otitis externa, hearing loss, earache, tinnitus, inner ear infection, deafness, ear fullness, ear pain, perforated ear drum, sensitivity to noise, Eustachian tube dysfunction, labyrinthitis, tongue disorder, taste perversion, taste loss, unusual taste, odd smell.


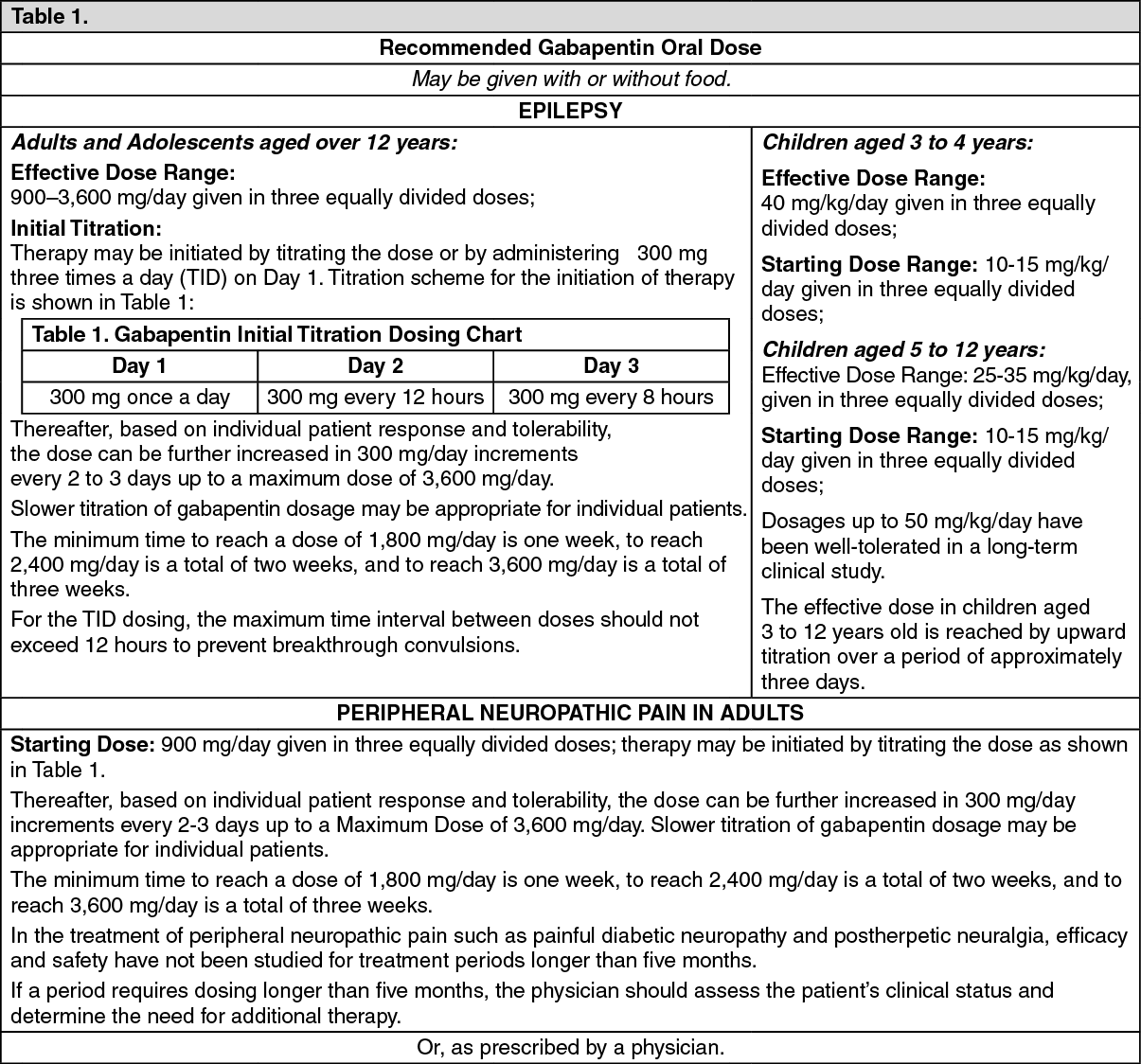 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image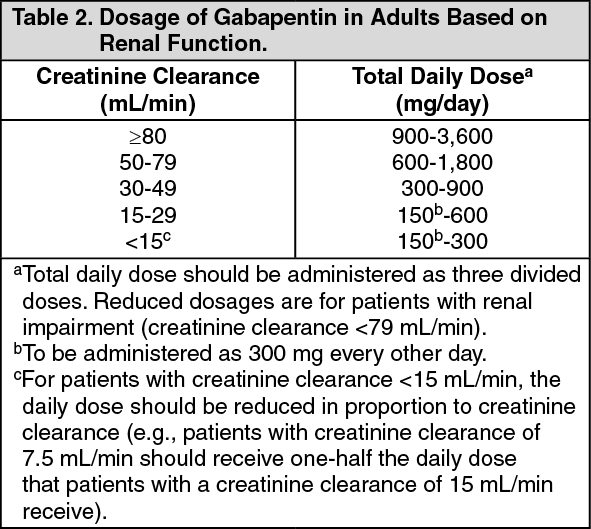 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out