275 mg: Each film-coated tablet contains: Naproxen Sodium 275 mg (equivalent to Naproxen 250 mg).
Naproxen Sodium (Sarimax) is a film-coated tablet which contains Naproxen Sodium, a Non-Steroidal Anti-Inflammatory Drug.
550 mg: Each film-coated Tablet contains: Naproxen Sodium 550 mg (equivalent to 500 mg of Naproxen).
550 mg: Pharmacotherapeutic group: Musculo-skeletal system, anti-inflammatory and anti-rheumatic products, non-steroids, propionic acid derivative. ATC code: MO1A E02.
Pharmacology: Pharmacodynamics: Naproxen belongs to the group of (non-aspirin) non-steroidal anti-inflammatory drugs which through reversible inhibition of the prostaglandin synthesis exert analgesic, antipyretic and anti-inflammatory functions. Naproxen is a non-selective COX inhibitor, it works by inhibiting both the COX-1 and COX-2 enzymes. It inhibits the formation of COX-1 dependent thromboxane synthase, A2 (TXA2), which reduces platelet aggregation, and the COX-2 dependent prostacyclin, (PGI2), which is an important vasodilatory mediator. Naproxen provides pain relief, lowers the fever and reduces the inflammatory response.
Pharmacokinetics: Naproxen sodium promptly dissolves in the gastric medium and is rapidly and completely absorbed from the gastrointestinal tract. Significant naproxen plasma levels and onset of pain relief can be obtained within 20 minutes of intake and peak levels (Cmax) are attained in about 1 hour (tmax).
Naproxen sodium extended release 660 mg is a bi-layer tablet with an immediate-release layer and an extended-release layer. The immediate-release layer starts to dissolve immediately while the extended-release layer dissolves slowly in the gastrointestinal tract. Peak levels (Cmax) are attained in about 45-60 minutes (tmax) under fasting conditions.
Following absorption, more than 99% is bound to serum albumin. The volume of distribution is app. 0.1 L/kg and the elimination half-life (t R1/2R) app. 14 hours. Naproxen is, after hepatic metabolism, primarily (≥ 95%) excreted through the kidneys. The pharmacokinetic data show linearity in the recommended dosage. Patients with severe hepatic impairment may have higher free naproxen levels. In severe renal insufficiency naproxen elimination is impaired, but no significant accumulation has been observed at the recommended dosage.
Toxicology: Preclinical Safety Data: Naproxen as other NSAIDs produce delayed parturition in animals.
Naproxen Sodium is used in musculoskeletal and joint disorders such as ankylosing spondylitis, osteoarthritis, and rheumatoid arthritis including juvenile idiopathic arthritis. It is also used in dysmenorrhea, headache including migraine, postoperative pain, soft tissue disorders, acute gout, and to reduce fever.
Method of Administration: Each dose should be taken orally with a glass of water, and can be taken fasting or with meals. Absorption may be delayed with meals.
Dosage Regimen: 275 mg: 1 tablet every 6-8 hours or 1 tablet every 12 hours.
The maximum daily dose of naproxen base equivalent should not exceed 800 mg (equivalent to 880 mg naproxen sodium). A daily dose (24 hours) of 800 mg naproxen base equivalent should not be exceeded unless otherwise directed by a health care professional or authorized by a local health authority.
Undesirable effects may be minimized by using the minimum effective dose for the shortest duration necessary to control symptoms.
Naproxen sodium must not be taken for more than ten days, unless under the direction of a doctor. If pain or fever persists or if symptoms change, a doctor should be consulted.
550 mg: 1 tablet every 24 hours.
Additional Information on Special Populations: Pediatric Patients: Children under 12 should not take this product, unless directed by a doctor.
Geriatric Patients: As elderly are more prone to side effects a lower dosage should be considered.
Patients with Severe Renal, Hepatic or Cardiac Impairment: In patients with severe, renal, hepatic and/or cardiac impairment dose reduction may be necessary.
Missed dose: 275 mg: Used the missed dose as soon as remembered but skip if it's almost time for the next scheduled dose.
Significant overdosage can be characterized by dizziness, drowsiness, epigastric pain, abdominal discomfort, heartburn, indigestion, nausea and vomiting, transient alterations in liver function, hypoprothrombinemia, renal dysfunction, metabolic acidosis, apnea, or disorientation. Because naproxen sodium may be rapidly absorbed, high and early blood levels should be anticipated. A few patients have experienced convulsions but it is not clear if these were naproxen related or not. Some cases with acute, reversible renal failure have been described. It is not known what dose of the drug would be life threatening.
Should a patient ingest a large quantity of naproxen sodium/naproxen the stomach may be emptied and usual supportive measures like administration of activated charcoal employed. Hemodialysis does not decrease the plasma concentration of naproxen because of the high degree of its protein binding. There is no specific antidote.
Known hypersensitivity to naproxen or any other ingredient in the drug product.
History of asthma, urticaria or allergic-type reactions after taking aspirin or other non-steroidal anti-inflammatory drugs (NSAIDs).
History of gastrointestinal bleeding or perforation related to previous NSAID therapy.
Active, or a history of, recurrent peptic ulcer or haemorrhage (two or more distinct episodes of proven ulceration or bleeding).
Severe heart failure.
Pain of gastrointestinal origin is not an indication for naproxen sodium/naproxen.
General Warnings: The use of naproxen sodium/naproxen with concomitant NSAIDs including cyclooxygenase-2 selective inhibitors should be avoided.
Undesirable effects may be minimised by using the lowest effective dose for the shortest duration necessary to control symptoms.
Gastrointestinal bleeding, ulceration and perforation: GI bleeding, ulceration or perforation, which can be fatal, has been reported with all NSAIDs at any time during treatment, with or without warning symptoms or a previous history of serious GI events. The risk of GI bleeding, ulceration or perforation is higher with increasing NSAID doses, in patients with a history of ulcer, particularly if complicated with haemorrhage or perforation, and in the elderly. These patients should commence treatment on the lowest dose available. Combination therapy with protective agents (e.g. misoprostol or proton pump inhibitors) should be considered for these patients, and also for patients requiring concomitant low dose aspirin, or other drugs likely to increase gastrointestinal risk.
Patients with a history of GI toxicity, particularly when elderly, should report any unusual abdominal symptoms (especially GI bleeding) particularly in the initial stages of treatment. Caution should be advised in patients receiving concomitant medications which could increase the risk of ulceration or bleeding, such as oral corticosteroids, anticoagulants such as warfarin, selective serotonin-reuptake inhibitors or anti-platelet agents such as aspirin.
When GI bleeding or ulceration occurs in patients receiving naproxen sodium/naproxen, the treatment should be withdrawn.
NSAIDs should be given with care to patients with a history of gastrointestinal disease (ulcerative colitis, Crohn's disease) as the condition may be exacerbated.
Sodium/fluid retention in cardiovascular conditions and peripheral edema: Caution (discussion with doctor or pharmacist) is required prior to starting treatment in patients with a history of hypertension and/or heart failure as fluid retention, hypertension and oedema have been reported in association with NSAID therapy.
Cardiovascular and cerebrovascular effects: Clinical trial and epidemiological data suggest that use of coxibs and some NSAIDs (particularly at high doses and in long term treatment) may be associated with a small increased risk of arterial thrombotic events (for example myocardial infarction or stroke). Although data suggest that the use of naproxen (1000 mg daily) may be associated with a lower risk, some risk cannot be excluded. There are insufficient data regarding the effects of low dose (naproxen sodium 220 mg-660 mg daily or naproxen 200 mg-600 mg daily) to draw firm conclusions on possible thrombotic risks.
Naproxen may attenuate acetylsalicylic acid's antiplatelet effect. Patients should talk to the doctor if they are on an acetylsalicylic acid regimen and plan to take naproxen sodium/naproxen.
Skin reactions: Serious skin reactions, some of them fatal, including exfoliative dermatitis, Stevens-Johnson syndrome, and toxic epidermal necrolysis, have been reported very rarely in association with the use of NSAIDs. Patients appear to be at highest risk of these reactions early in the course of therapy.
Naproxen sodium/naproxen should be discontinued at the first appearance of skin rash, mucosal lesions, or any other sign of hypersensitivity.
Anaphylactic (anaphylactoid) reactions: Hypersensitivity reactions, including anaphylactic (anaphylactoid) reactions may occur both in patients with and without a history of hypersensitivity on exposure to aspirin, other non-steroidal anti-inflammatory drugs or naproxen-containing products. They may also occur in individuals with a history of angioedema, bronchospastic reactivity (e.g. asthma), rhinitis, nasal polyps, allergic disease, chronic respiratory disease or aspirin sensitivity. This also applies to patients exhibiting allergic reactions (e.g. cutaneous reactions, itching urticaria) to naproxen or other NSAIDs. Anaphylactoid reactions, like anaphylaxis, may have a fatal outcome.
Hepatic effects: Severe hepatic reactions, including jaundice and hepatitis (some cases of hepatitis have been fatal), have been reported with naproxen sodium/naproxen as with other non-steroidal anti-inflammatory drugs. Cross reactivity has been reported.
Special Populations: Women who are pregnant or plan to become pregnant: Precautions related to fertility: There is some evidence that drugs which inhibit cyclooxygenase/prostaglandin synthesis may cause impairment of female fertility by an effect on ovulation. This is reversible on withdrawal of treatment.
Patients with medical history: Subjects with the following additional medical history should be under adequate and careful supervision of the doctor when taking naproxen sodium/naproxen: who are taking any other analgesic; who are taking steroids; with coagulation disturbances or who take drugs that influence hemostasis; on intensive diuretic therapy; with severe renal, hepatic, or cardiac impairment.
Effects on Ability to Drive and Use Machines: No studies on the effect on the ability to drive and use machines have been performed. However, undesirable effects such as drowsiness, dizziness, vertigo, insomnia have been observed with the use of naproxen sodium/naproxen. Patients should be cautioned to see how they react before driving or operating machinery.
Use in Elderly: Elderly have an increased frequency of adverse reactions to NSAIDs especially gastrointestinal bleeding and perforation which may be fatal.
275 mg: Consult the Doctor: If pain or fever persists or if symptoms change, a doctor should be consulted.
550 mg: Pregnancy: As with other drugs of this type, naproxen sodium/naproxen produces delay in parturition in animals and also affects the human foetal cardiovascular system (closure of the ductus arteriosus). Therefore, naproxen sodium/naproxen should not be used unless clearly needed and directed to do so by a doctor. The use of naproxen sodium/naproxen in pregnancy requires cautious balancing of the possible benefits against potential risk to the mother and foetus, especially during the first and third trimester.
Lactation: Naproxen has been found in the milk of lactating mothers. The use of naproxen sodium/naproxen should therefore be avoided in women who are breast feeding.
Fertility: There is some evidence that drugs which inhibit cyclooxygenase/prostaglandin synthesis may cause impairment of female fertility by an effect on ovulation. This is reversible on withdrawal of treatment.
Cardiac Disorders/Vascular Disorders: Oedema, hypertension, and cardiac failure, have been reported in association with NSAID treatment. Clinical trial and epidemiological data suggest that use of coxibs and some NSAIDs (particularly at high doses and in long term treatment) may be associated with a small increased risk of arterial thrombotic events (for example myocardial infarction or stroke).
Gastrointestinal Disorders: The most commonly observed adverse events are gastrointestinal in nature. Peptic ulcers, perforation or GI bleeding, sometimes fatal, particularly in the elderly, may occur. Nausea, vomiting, diarrhoea, flatulence, constipation, dyspepsia, abdominal pain, melena, hematemesis, ulcerative stomatitis, exacerbation of colitis and Crohn's disease have been reported following administration. Less frequently, gastritis has been observed.
Skin and Subcutaneous Tissue Disorders: Bullous reactions including Stevens-Johnson syndrome and toxic epidermal necrolysis (very rare). Naproxen causes transient, dose-dependent modestly increased bleeding times. However, these values often do not exceed the upper limit of the reference range.
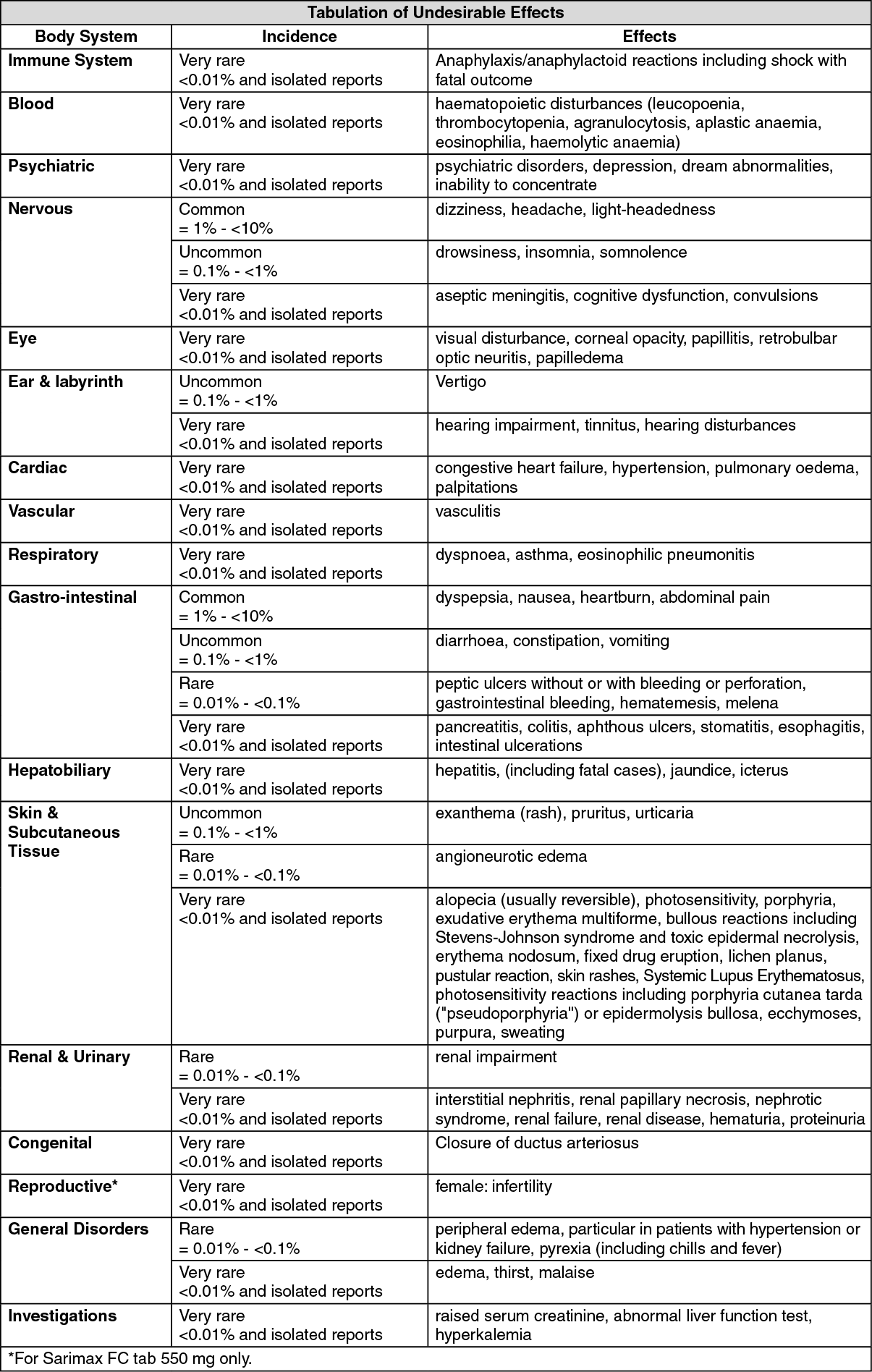
Tabulation of Undesirable Effects: The following adverse drug reactions have been observed for naproxen or naproxen sodium products, including those with prescription dosing. (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Cyclosporine: Cyclosporine concentrations may increase, increasing the risk for nephrotoxicity.
Lithium: Lithium levels may increase, which could induce nausea, polydipsia, polyuria, tremor, confusion.
Methotrexate used at doses of 15 mg/week or more: Elevated concentration of methotrexate, increasing the risk for toxicity to this substance.
Non-steroidal anti-inflammatory drugs (NSAIDs) including aspirin: Increased risk of ulcers and gastrointestinal bleeding.
Low-dose aspirin: Naproxen may attenuate the irreversible platelet inhibition induced by acetylsalicylic acid. Clinical pharmacodynamic data suggest that concurrent (same day) naproxen sodium/naproxen usage for more than one day consecutively inhibits the effect of low-dose acetylsalicylic acid on platelet activity and this inhibition may persist for up to several days after stopping naproxen sodium/naproxen therapy. The clinical relevance of this interaction is not known. Treatment with naproxen/naproxen sodium in patients with increased cardiovascular risk may limit the cardiovascular protection of acetylsalicylic acid.
Anticoagulants: NSAIDs may enhance the effects of anti-coagulants, such as warfarin. Anticoagulants and other drugs influencing hemostasis add to the risk of bleeding and require careful monitoring.
Anti-platelet agents and selective serotonin reuptake inhibitors (SSRIs): Increased risk of gastrointestinal bleeding.
Corticosteroids: Increased risk of gastro-intestinal ulceration or bleeding.
Diuretics and antihypertensive drugs including ACE Inhibitors: The diuretic and antihypertensive efficacy, particularly in patients with pre-existing nephropathy, may be reduced.
During short term use of naproxen sodium/naproxen interactions of clinical significance do not seem to be relevant for the following medications: Antacids; Antidiabetic agents; Hydantoins; Probenecid; Zidovudine.
Drug-Food Interaction: The absorption may be delayed with a meal.
Interference with Laboratory Testing: Naproxen sodium/naproxen has been claimed to interfere with the urinary analyses of 17-ketogenic steroids and 5-hydroxy indoleacetic acid (5 HIAA).
Special Precautions for Disposal and Other Handling: No special requirements.
Store at temperatures not exceeding 25°C.
M01AE02 - naproxen ; Belongs to the class of propionic acid derivatives of non-steroidal antiinflammatory and antirheumatic products.
Sarimax FC tab 275 mg
100's (P10.75/film-coated tab)
Sarimax FC tab 550 mg
100's (P20.25/film-coated tab)


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out