


 Sign Out
Sign Out

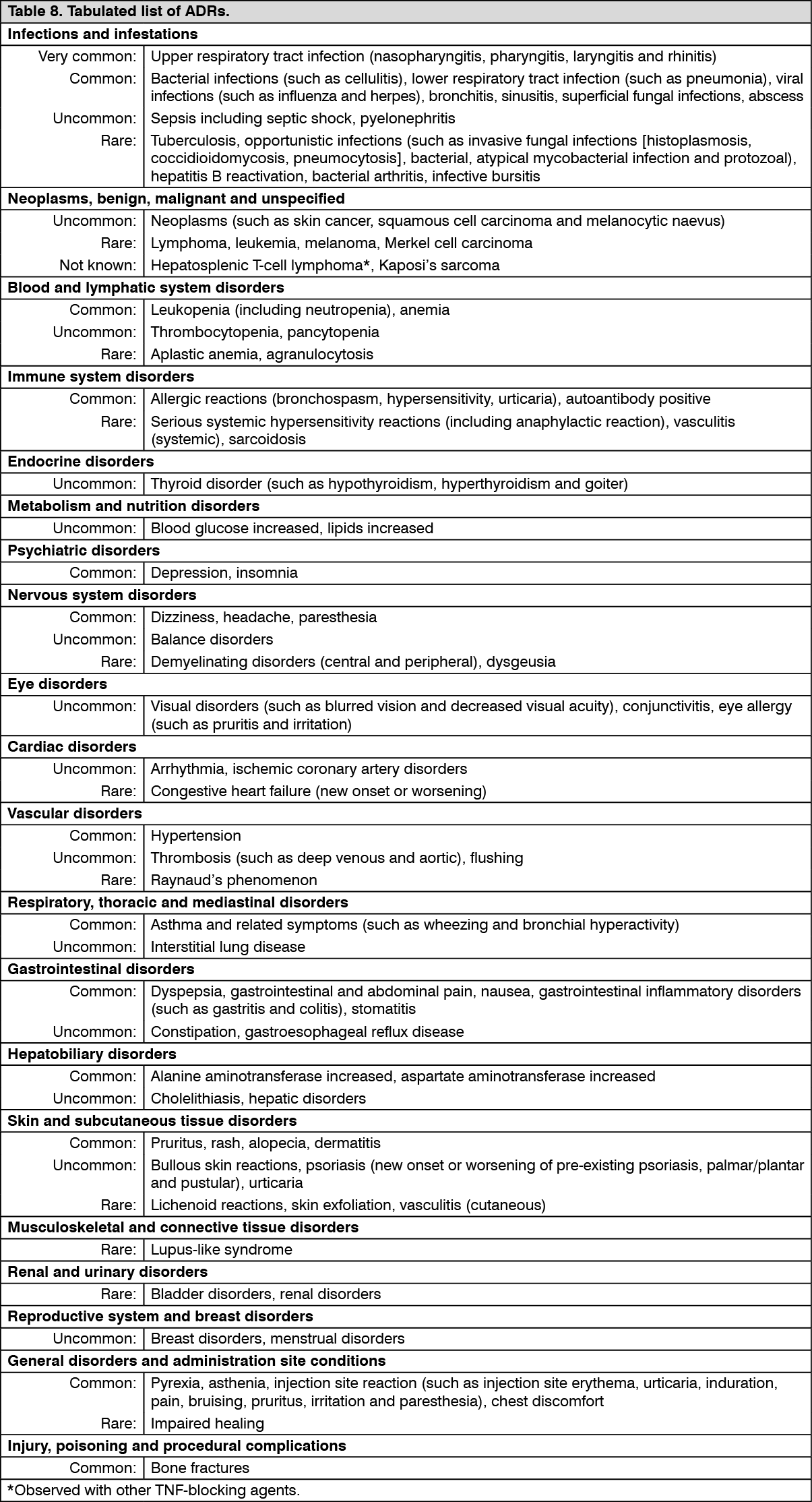
Tabulated list of adverse reactions: ADRs observed in clinical studies and reported from world‑wide post‑marketing use of golimumab are listed in Table 8. Within the designated system organ classes, the adverse drug reactions are listed under headings of frequency and using the following convention: very common (≥ 1/10); common (≥ 1/100 to < 1/10); uncommon (≥ 1/1,000 to < 1/100); rare (≥ 1/10,000 to < 1/1,000); very rare (< 1/10,000); not known (cannot be estimated from the available data). Within each frequency grouping, adverse reactions are presented in order of decreasing seriousness. (See Table 8.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThroughout this section, median duration of follow-up (approximately 4 years) is generally presented for all golimumab use. Where golimumab use is described by dose, the median duration of follow-up varies (approximately 2 years for 50 mg dose, approximately 3 years for 100 mg dose) as patients may have switched between doses.
Description of selected adverse drug reactions: Infections: In the controlled period of pivotal trials, upper respiratory tract infection was the most common adverse reaction reported in 12.6% of golimumab‑treated patients (incidence per 100 subject‑years: 60.8; 95% CI: 55.0, 67.1) compared with 11.0% of control patients (incidence per 100 subject‑years: 54.5; 95% CI: 46.1, 64.0). In controlled and uncontrolled portions of the studies with a median follow‑up of approximately 4 years, the incidence per 100 subject‑years of upper respiratory tract infections was 34.9 events; 95% CI: 33.8, 36.0 for golimumab treated patients.
In the controlled period of pivotal trials, infections were observed in 23.0% of golimumab‑treated patients (incidence per 100 subject‑years: 132.0; 95% CI: 123.3, 141.1) compared with 20.2% of control patients (incidence per 100 subject‑years: 122.3; 95% CI: 109.5, 136.2). In controlled and uncontrolled portions of the trials with a median follow‑up of approximately 4 years, the incidence per 100 subject‑years of infections was 81.1 events; 95% CI: 79.5, 82.8 for golimumab treated patients.
In the controlled period of RA, PsA, AS, and nr‑Axial SpA trials, serious infections were observed in 1.2% of golimumab‑treated patients and 1.2% of control‑treated patients. The incidence of serious infections per 100 subject‑years of follow‑up in the controlled period of RA, PsA, AS, and nr‑Axial SpA trials was 7.3; 95% CI: 4.6, 11.1 for the golimumab 100 mg group, 2.9; 95% CI: 1.2, 6.0 for the golimumab 50 mg group and 3.6; 95% CI: 1.5, 7.0 for the placebo group. In the controlled period of UC trials of golimumab induction, serious infections were observed in 0.8% of golimumab-treated patients compared with 1.5% of control-treated patients. Serious infections observed in golimumab‑treated patients included tuberculosis, bacterial infections including sepsis and pneumonia, invasive fungal infections and other opportunistic infections. Some of these infections have been fatal. In the controlled and uncontrolled portions of the pivotal trials with a median follow‑up of up to 3 years, there was a greater incidence of serious infections, including opportunistic infections and TB in patients receiving golimumab 100 mg compared with patients receiving golimumab 50 mg. The incidence per 100 subject‑years of all serious infections was 4.1; 95% CI: 3.6, 4.5, in patients receiving golimumab 100 mg and 2.5; 95% CI: 2.0, 3.1, in patients receiving golimumab 50 mg.
Malignancies: Lymphoma: The incidence of lymphoma in golimumab-treated patients during the pivotal trials was higher than expected in the general population. In the controlled and uncontrolled portions of these trials with a median follow‑up of up to 3 years, a greater incidence of lymphoma was observed in patients receiving golimumab 100 mg compared with patients receiving golimumab 50 mg. Lymphoma was diagnosed in 11 subjects (1 in the golimumab 50 mg treatment groups and 10 in the golimumab 100 mg treatment groups) with an incidence (95% CI) per 100 subject‑years of follow-up of 0.03 (0.00, 0.15) and 0.13 (0.06, 0.24) events for golimumab 50 mg and 100 mg respectively and 0.00 (0.00, 0.57) events for the placebo.
The majority of lymphomas occurred in study GO‑AFTER, which enrolled patients previously exposed to anti‑TNF agents who had longer disease duration and more refractory disease (see Precautions).
Malignancies other than lymphoma: In the controlled periods of pivotal trials and through approximately 4 years of follow‑up, the incidence of non‑lymphoma malignancies (excluding non‑melanoma skin cancer) was similar between the golimumab and the control groups. Through approximately 4 years of follow-up, the incidence of non-lymphoma malignancies (excluding non-melanoma skin cancer) was similar to the general population.
In the controlled and uncontrolled periods of pivotal trials with a median follow-up of up to 3 years, non-melanoma skin cancer was diagnosed in 5 placebo-treated, 10 golimumab 50 mg-treated and 31 golimumab 100 mg-treated subjects with an incidence (95% CI) per 100 subject‑years of follow-up of 0.36 (0.26, 0.49) for combined golimumab and 0.87 (0.28, 2.04) for placebo.
In the controlled and uncontrolled period of pivotal trials with a median follow-up of up to 3 years, malignancies besides melanoma, non-melanoma skin cancer and lymphoma were diagnosed in 5 placebo-treated, 21 golimumab 50 mg-treated and 34 golimumab 100 mg-treated subjects with an incidence (95% CI) per 100 subject‑years of follow‑up of 0.48 (0.36, 0.62) for combined golimumab and 0.87 (0.28, 2.04) for placebo (see Precautions).
Cases reported in clinical studies in asthma: In an exploratory clinical study, patients with severe persistent asthma received a golimumab loading dose (150% of the assigned treatment dose) subcutaneously at week 0 followed by golimumab 200 mg, golimumab 100 mg or golimumab 50 mg every 4 weeks subcutaneously through week 52. Eight malignancies in the combined golimumab treatment group (n = 230) and none in the placebo treatment group (n = 79) were reported. Lymphoma was reported in 1 patient, non‑melanoma skin cancer in 2 patients, and other malignancies in 5 patients. There was no specific clustering of any type of malignancy.
During the placebo‑controlled portion of the study, the incidence (95% CI) of all malignancies per 100 subject‑years of follow‑up was 3.19 (1.38, 6.28) in the golimumab group. In this study, the incidence (95% CI) per 100 subject‑years of follow‑up in golimumab‑treated subjects was 0.40 (0.01, 2.20) for lymphoma, 0.79 (0.10, 2.86) for non‑melanoma skin cancers, and 1.99 (0.64, 4.63) for other malignancies. For placebo subjects, the incidence (95% CI) per 100 subject‑years of follow‑up of these malignancies was 0.00 (0.00, 2.94). The significance of this finding is unknown.
Neurological events: In the controlled and uncontrolled periods of the pivotal trials with a median follow‑up of up to 3 years, a greater incidence of demyelination was observed in patients receiving golimumab 100 mg compared with patients receiving golimumab 50 mg (see Precautions).
Liver enzyme elevations: In the controlled period of RA and PsA pivotal trials, mild ALT elevations (> 1 and < 3 x upper limit of normal (ULN)) occurred in similar proportions of golimumab and control patients in the RA and PsA studies (22.1% to 27.4% of patients); in the AS and nr‑Axial SpA studies, more golimumab‑treated patients (26.9%) than control patients (10.6%) had mild ALT elevations. In the controlled and uncontrolled periods of the RA and PsA pivotal trials, with a median follow-up of approximately 5 years, the incidence of mild ALT elevations was similar in golimumab‑treated and control patients in RA and PsA studies. In the controlled period of the UC pivotal trials of golimumab induction, mild ALT elevations (> 1 and < 3 x ULN) occurred in similar proportions of golimumab‑treated and control patients (8.0% to 6.9%, respectively). In controlled and uncontrolled periods of the UC pivotal trials with a median follow-up of approximately 2 years, the proportion of patients with mild ALT elevations was 24.7% in patients receiving golimumab during the maintenance portion of the UC study.
In the controlled period of RA and AS pivotal trials, ALT elevations ≥ 5 x ULN were uncommon and seen in more golimumab‑treated patients (0.4% to 0.9%) than control patients (0.0%). This trend was not observed in the PsA population. In the controlled and uncontrolled periods of RA, PsA and AS pivotal trials, with a median follow-up of 5 years, the incidence of ALT elevations ≥ 5 x ULN was similar in both golimumab‑treated and control patients. In general these elevations were asymptomatic and the abnormalities decreased or resolved with either continuation or discontinuation of golimumab or modification of concomitant medicinal products. No cases were reported in the controlled and uncontrolled periods of the nr‑Axial SpA study (up to 1 year). In the controlled periods of the pivotal UC trials, of golimumab induction, ALT elevations ≥ 5 x ULN occurred in similar proportions of golimumab‑treated patients compared to placebo-treated patients (0.3% to 1.0%, respectively). In the controlled and uncontrolled periods of the pivotal UC trials with a median follow-up of approximately 2 years, the proportion of patients with ALT elevations ≥ 5 x ULN was 0.8% in patients receiving golimumab during the maintenance portion of the UC study.
Within the RA, PsA, AS, and nr‑Axial SpA pivotal trials, one patient in an RA trial with pre‑existing liver abnormalities and confounding medicinal products treated with golimumab developed non‑infectious fatal hepatitis with jaundice. The role of golimumab as a contributing or aggravation factor cannot be excluded.
Injection site reactions: In the controlled periods of pivotal trials, 5.4% of golimumab‑treated patients had injection site reactions compared with 2.0% in control patients. The presence of antibodies to golimumab may increase the risk of injection site reactions. The majority of the injection site reactions were mild and moderate and the most frequent manifestation was injection site erythema. Injection site reactions generally did not necessitate discontinuation of the medicinal product.
In controlled Phase IIb and/or III trials in RA, PsA, AS, nr‑Axial SpA, severe persistent asthma, and Phase II/III trials in UC, no patients treated with golimumab developed anaphylactic reactions.
Autoimmune antibodies: In the controlled and uncontrolled periods of pivotal trials through 1 year of follow-up, 3.5% of golimumab‑treated patients and 2.3% of control patients were newly ANA‑positive (at titres of 1:160 or greater). The frequency of anti‑dsDNA antibodies at 1 year of follow-up in patients anti‑dsDNA negative at baseline was 1.1%.
Pediatric population: Polyarticular juvenile idiopathic arthritis: The safety of golimumab has been studied in a phase III study of 173 pJIA patients from 2 to 17 years of age. The average follow-up was approximately two years. In this study, the type and frequency of adverse events reported were generally similar to those seen in adult RA studies.
View ADR Monitoring Form