


 Sign Out
Sign Out

Clinical trial data: Adverse Reactions from Clinical Studies in Treatment‑Resistant Depression (TRD): Esketamine (Spravato) was evaluated for safety in 1709 patients diagnosed with TRD (patients with MDD and were non‑responders to at least two oral antidepressants (ADs) treatments, of adequate dosage and duration, in the current major depressive episode) from five Phase 3 studies (3 short‑term and 2 long‑term studies) and one Phase 2 dose‑ranging study. Of all esketamine‑treated patients in the completed Phase 3 studies, 479 (29.9%) received at least 6 months of treatment exposure, and 178 (11.1%) received at least 12 months of exposure.
Adverse reactions in patients with Major Depressive Disorder with acute suicidal ideation or behavior: Esketamine (Spravato) was evaluated for safety in 262 patients diagnosed with Major Depressive Disorder with suicidal ideation and intent from two Phase 3 studies and one Phase 2 study. Overall, the safety profile of Esketamine (Spravato) from this clinical program was generally similar that seen in studies for TRD.
Adverse Events Reported as Reasons for Discontinuation of Treatment: In short‑term studies in both adult (pooled TRD3001/TRD3002) and elderly (TRD3005) patients with TRD, the proportion of patients that received Esketamine (Spravato) plus oral AD and discontinued treatment because of an adverse event was 4.6% for adult and 5.6% for elderly patients, respectively, compared to 1.4% for adult and 3.1% for elderly patients receiving oral AD plus placebo nasal spray. In a long‑term study, the discontinuation rates because of an adverse event were similar for patients receiving Esketamine (Spravato) plus oral AD and oral AD plus placebo nasal spray, 2.6% and 2.1%, respectively. Across all Phase 3 studies in TRD, adverse events leading to Esketamine (Spravato) discontinuation in more than 2 patients (>0.1%) were (in order of frequency): anxiety, depression, blood pressure increased, dizziness, suicidal ideation, dissociation, nausea, vomiting, headache, muscular weakness, vertigo, hypertension, panic attack and sedation.
In the pooled Phase 3 studies SUI3001/SUI3002, 6.2% (14/227) of patients diagnosed with Major Depressive Disorder with suicidal ideation and intent in the Esketamine (Spravato) + SOC group and 3.6% (8/225) of patients in the placebo + SOC group experienced adverse events leading to discontinuation. Adverse events that led to discontinuation in >1 subject in the Esketamine (Spravato) + SOC group were: dissociation, blood pressure increased, depersonalization/derealization disorder, and nausea.
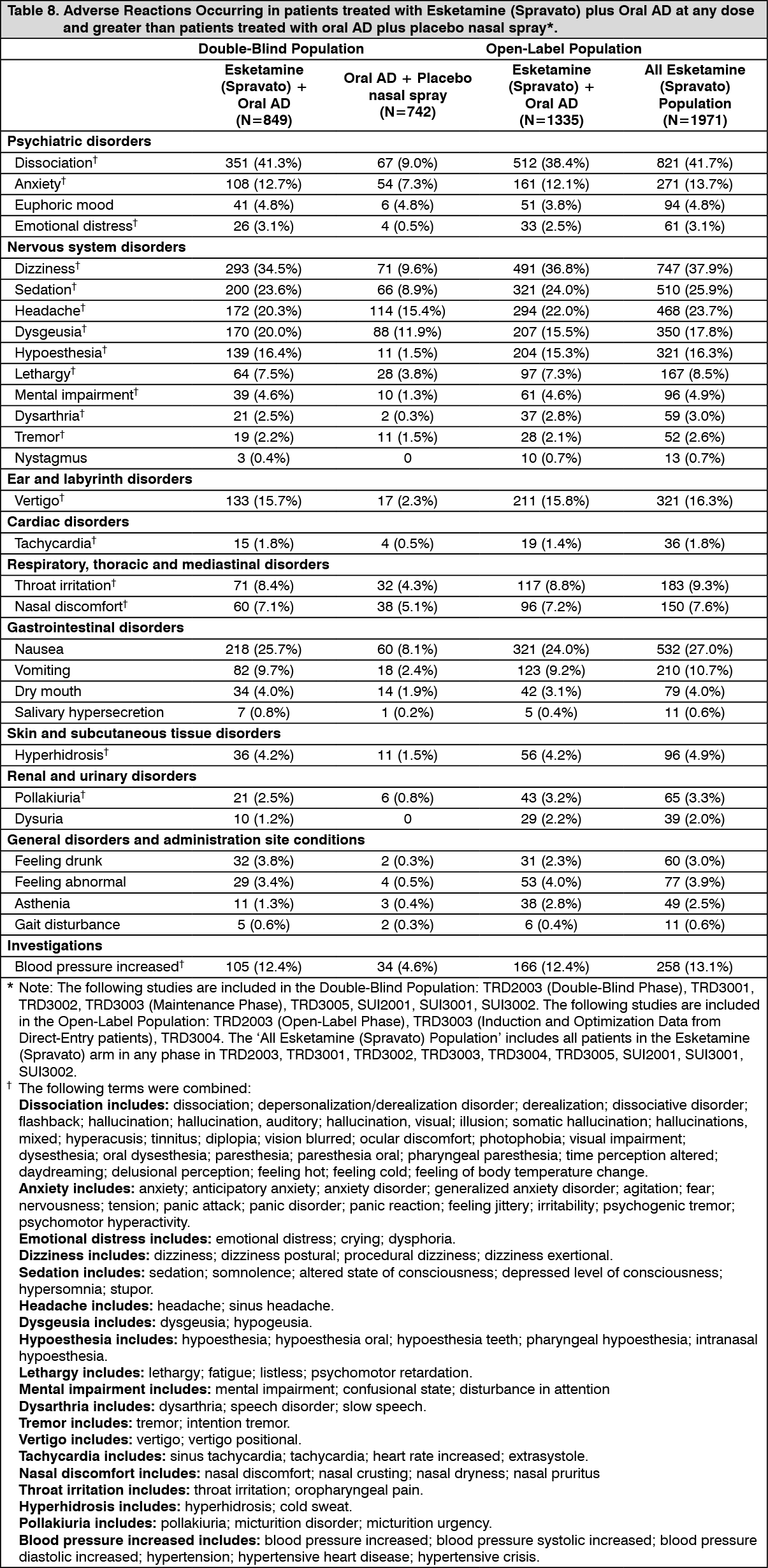
Common Adverse Reactions: The most commonly observed adverse reactions in patients treated with Esketamine (Spravato) plus oral AD (incidence ≥10% and greater than oral AD plus placebo nasal spray) were dissociation, dizziness, nausea, sedation, headache, dysgeusia, hypoesthesia, vertigo, anxiety, blood pressure increased, and vomiting. Most of these adverse reactions were mild or moderate in severity, reported post‑dose on the day of administration and resolved the same day.
Table 8 shows the incidence of adverse reactions that occurred in patients treated with Esketamine (Spravato) plus oral AD at any dose and greater than patients treated with oral AD plus placebo nasal spray. (See Table 8.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDissociation/perceptual changes: The most common psychological effects of esketamine have been dissociative/perceptual changes (including distortion of time and space and illusions), derealization and depersonalization. These adverse reactions were reported as transient and self‑limited and occurred on the day of dosing. Dissociation was reported as severe in intensity at the incidence of less than 4% across studies. Dissociation symptoms typically resolved by 1.5 hours post‑dose and the severity tended to reduce over time with repeated treatments.
Sedation/somnolence: Adverse reactions of sedation and somnolence were primarily mild or moderate in severity, occurred on the day of dosing and resolved spontaneously the same day. Sedative effects typically resolved by 1.5 hours post-dose. Rates of somnolence were relatively stable over time during long-term treatment. In the cases of sedation, no symptoms of respiratory distress were observed, and hemodynamic parameters (including vital signs and oxygen saturation) remained within normal ranges. During post-marketing use, respiratory depression has been observed in isolated cases with the use of Esketamine (Spravato) in combination with other CNS depressants and in patients with comorbidities such as obesity, anxiety, cardiovascular and respiratory conditions, though causality has not been established. These events were transient in nature and resolved after verbal/tactile stimulation or supplemental oxygen.
Impaired cognition: In the short‑term studies, treatment with Esketamine (Spravato) plus oral AD did not influence any aspect of cognition studied in adult patients with TRD and was not associated with any systematic changes in cognition in the elderly patients. Consistently, in long‑term studies, performance on each of the cognitive tests relative to baseline showed slight improvement or remained stable in each treatment phase. In the elderly subgroup (≥65 years of age) slowing of reaction time starting at Week 20 and through the end of the study was observed, however, performance on other cognitive tests remained stable.
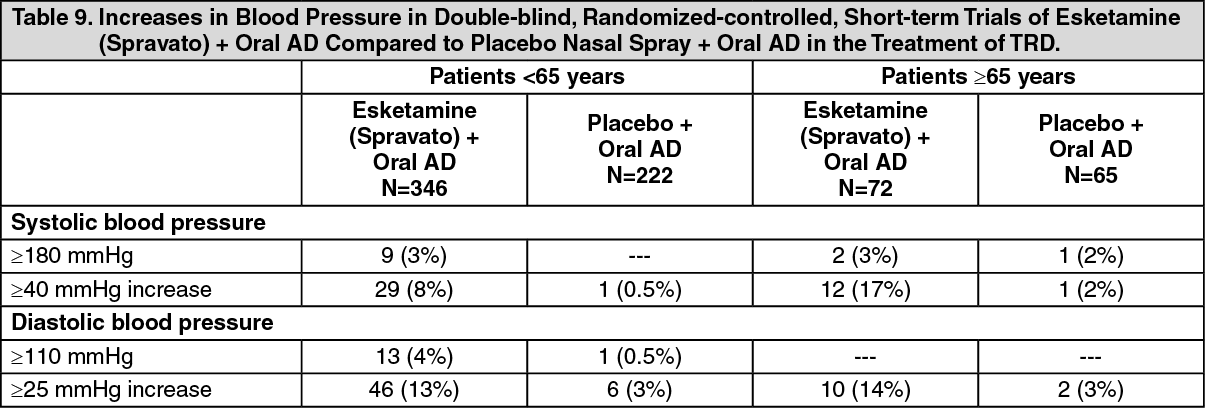
Changes in blood pressure: The mean placebo-adjusted increases in systolic and diastolic blood pressure (SBP and DBP) over time were about 7 to 9 mmHg in SBP and 4 to 6 mmHg in DBP at 40 minutes post-dose and 2 to 5 mmHg in SBP and 1 to 3 mmHg in DBP at 1.5 hours post-dose in patients receiving Esketamine (Spravato) plus oral antidepressants. (See Table 9.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageNausea and vomiting: Esketamine (Spravato) can cause nausea and vomiting (Table 10). Most of these events occurred on the day of dosing and resolved the same day, with the median duration not exceeding 1 hour in most subjects across dosing sessions. Rates of reported nausea and vomiting decreased over time across dosing sessions from the first week of treatment in the short-term studies, as well as over time with long-term treatment. (See Table 10.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageNasal tolerability and sense of smell: Across studies, the vast majority of esketamine‑treated patients had no findings on nasal examination. For the patients who had nasal findings (including nasal discharge, nasal crust, or nasal erythema) all events were of mild severity with the exception of a few moderate findings. The most frequently reported post‑dose nasal symptoms of moderate or severe intensity (reported in at least 5% of patients) in the Phase 3 studies were post‑nasal drip, taste disturbance and stuffy nose. Other nasal symptoms of moderate or severe intensity included: runny nose, cough, dryness inside nose and sneezing. In addition, sense of smell was assessed over time; no difference was observed between patients treated with Esketamine (Spravato) plus oral AD and those treated with oral AD plus placebo nasal spray during the double‑blind maintenance phase of TRD3003.
Body weight: Esketamine (Spravato) had no clinically meaningful effect on body weight over short‑ or long‑term administration. In the double‑blind maintenance phase of TRD3003, the proportion of patients with an increase in body weight of ≥7% was comparable for the Esketamine (Spravato) plus oral AD vs oral AD plus placebo nasal spray groups (13.9% and 13.3%). In the open‑label, long‑term study TRD3004, a similar percentage of patients exhibited an increase or decrease in body weight of ≥7% (7.4% and 9.1%, respectively). In TRD3004, mean body weight remained stable during treatment with Esketamine (Spravato) plus oral AD both in the induction phase and maintenance phase (mean change from baseline ± standard deviation of ‑0.29±2.15 kg at Day 28 and 0.44±5.83 kg at Week 48).
Laboratory values: Esketamine (Spravato) has not been associated with any clinically important changes to laboratory parameters in serum chemistry, hematology, or urinalysis.
View ADR Monitoring Form