


 Sign Out
Sign Out
New onset or worsening of renal impairment (see Precautions).
Lactic Acidosis/Severe Hepatomegaly with Steatosis (see Precautions).
Adverse Reactions in Adult Subjects with Chronic Hepatitis B and Compensated Liver Disease: The safety assessment of Tenofovir Alafenamide was based on pooled data through the Week 96 data analysis from 1298 subjects in two randomized, double-blind, active-controlled trials, Trial 108 and Trial 110, in adult subjects with chronic hepatitis B and compensated liver disease. A total of 866 subjects received Tenofovir Alafenamide 25 mg once daily. Further safety assessment was based on pooled data from Trials 108 and 110 from subjects who continued to receive their original blinded treatment through Week 120 and additionally from subjects who received open-label Tenofovir Alafenamide was from Week 96 through Week 120 (n=361 remained on Tenofovir Alafenamide; n=180 switched from TDF to Tenofovir Alafenamide at Week 96).
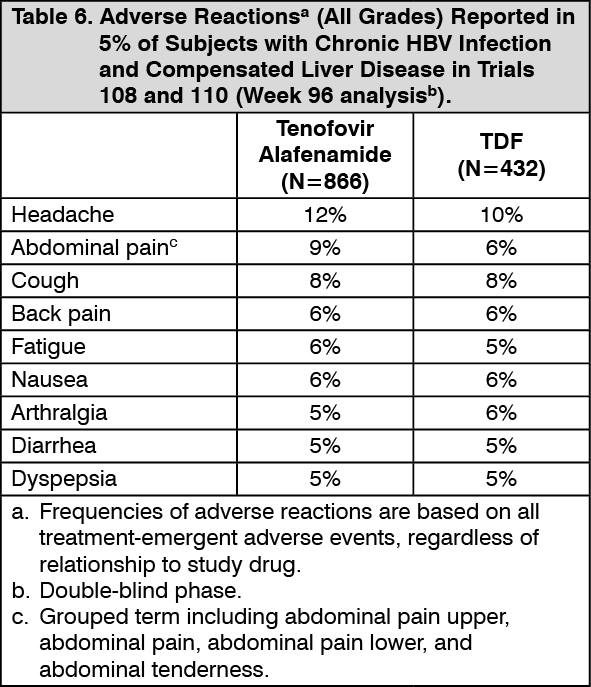
Based on the Week 96 analysis, the most common adverse reaction (all Grades) reported in at least 10% of subjects in the Tenofovir Alafenamide group was headache. The proportion of subjects who discontinued treatment with Tenofovir Alafenamide or TDF due to adverse reactions of any severity was 1.5% and 0.9%, respectively. Table 6 displays the frequency of the adverse reactions (all Grades) greater than or equal to 5% in the Tenofovir Alafenamide group. (See Table 6).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAdditional adverse reactions occurring in less than 5% of subjects in Trials 108 and 110 included vomiting, rash, and flatulence.
The safety profile of Tenofovir Alafenamide in subjects who continued to receive blinded treatment through Week 120 was similar to that at Week 96. The safety profile of Tenofovir Alafenamide in subjects who remained on Tenofovir Alafenamide in the open-label phase through Week 120 was similar to that in subjects who switched from TDF to Tenofovir Alafenamide at Week 96.
Renal Laboratory Tests: In a pooled analysis of Trials 108 and 110 in adult subjects with chronic hepatitis B and a median baseline estimated creatinine clearance between 106 and 105 mL per minute (for the Tenofovir Alafenamide and TDF groups, respectively), mean serum creatinine increased by less than 0.1 mg/dL and median serum phosphorus decreased by 0.1 mg/dL in both treatment groups at Week 96. Median change from baseline to Week 96 in estimated creatinine clearance was -1.2 mL per minute in the Tenofovir Alafenamide group and -4.8 mL per minute in those receiving TDF.
In subjects who remained on blinded treatment beyond Week 96 in Trials 108 and 110, change from baseline in renal laboratory parameter values in each group at Week 120 were similar to those at Week 96. In the open-label phase, median change in estimated creatinine clearance by Cockcroft-Gault method from Week 96 to Week 120 was -0.6 mL per minute in subjects who remained on Tenofovir Alafenamide and +1.8 mL per minute in those who switched from TDF to Tenofovir Alafenamide at Week 96. Mean serum creatinine and median serum phosphorus values at Week 120 were similar to those at Week 96 in subjects who remained on Tenofovir Alafenamide and in subjects who switched from TDF to Tenofovir Alafenamide.
The long-term clinical significance of these renal laboratory changes on adverse reaction frequencies between Tenofovir Alafenamide and TDF is not known.
Bone Mineral Density Effects: In a pooled analysis of Trials 108 and 110, the mean percentage change in bone mineral density (BMD) from baseline to Week 96 as assessed by dual-energy X-ray absorptiometry (DXA) was -0.7% with Tenofovir Alafenamide compared to -2.6% with TDF at the lumbar spine and -0.3% compared to -2.5% at the total hip. BMD declines of 5% or greater at the lumbar spine were experienced by 11% of Tenofovir Alafenamide subjects and 25% of TDF subjects at Week 96. BMD declines of 7% or greater at the femoral neck were experienced by 5% of Tenofovir Alafenamide subjects and 13% of TDF subjects at Week 96.
In subjects who remained on blinded treatment beyond Week 96 in Trials 108 and 110, mean percentage change in BMD in each group at Week 120 was similar to that at Week 96. In the open-label phase, mean percentage change in BMD from Week 96 to Week 120 in subjects who remained on Tenofovir Alafenamide was 0.6% at the lumbar spine and 0% at the total hip, compared to 1.7% at the lumbar spine and 0.6% at the total hip in those who switched from TDF to Tenofovir Alafenamide. The long-term clinical significance of these BMD changes is not known.
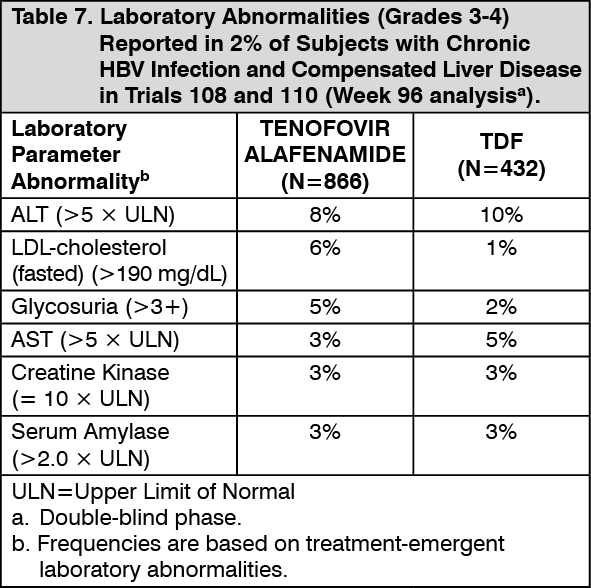
Laboratory Abnormalities: The frequency of laboratory abnormalities (Grades 3–4) occurring in at least 2% of subjects receiving Tenofovir Alafenamide in Trials 108 and 110 are presented in Table 7. (See Table 7).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe overall incidence of blinded treatment ALT flares (defined as confirmed serum ALT greater than 2 × baseline and greater than 10 × ULN at 2 consecutive postbaseline visits, with or without associated symptoms) was similar between Tenofovir Alafenamide (0.6%) and TDF (0.9%) through Week 96. ALT flares generally were not associated with coincident elevations in bilirubin, occurred within the first 12 weeks of treatment, and resolved without recurrence.
Based on the Week 120 analysis, the frequencies of lab abnormalities in subjects who remained on Tenofovir Alafenamide in the open-label phase were similar to those in subjects who switched from TDF to Tenofovir Alafenamide at Week 96.
Amylase and Lipase Elevations and Pancreatitis: At Week 96, in Trials 108 and 110, eight subjects treated with Tenofovir Alafenamide with elevated amylase levels had associated symptoms, such as nausea, low back pain; abdominal tenderness, pain, and distension; and biliary pancreatitis and pancreatitis. Of these eight, two subjects discontinued Tenofovir Alafenamide due to elevated amylase and/or lipase; one subject experienced recurrence of adverse events when Tenofovir Alafenamide was restarted. No subject treated with TDF had associated symptoms or discontinued treatment.
From Week 96 to Week 120, one additional subject who continued open-label Tenofovir Alafenamide and none of the subjects who switched from TDF to Tenofovir Alafenamide had elevated amylase levels and associated symptoms.
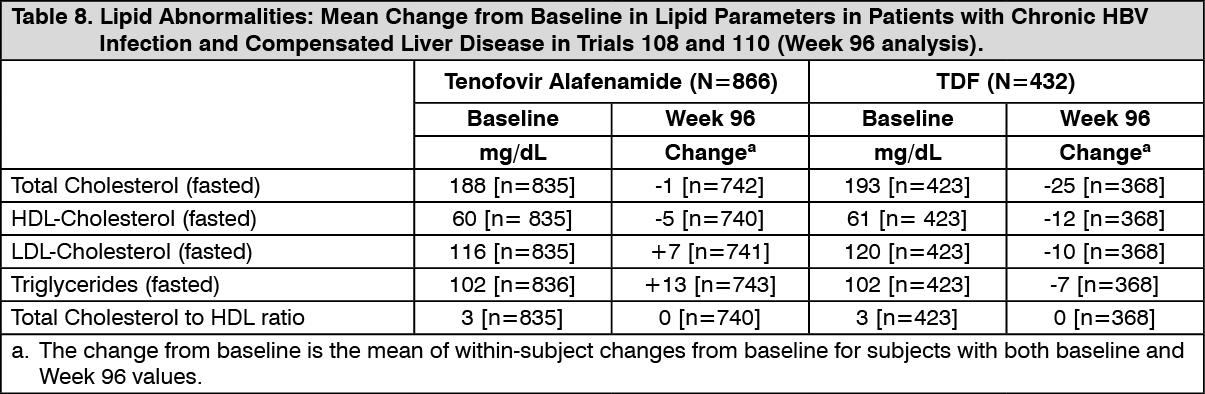
Serum Lipids: Changes from baseline in total cholesterol, HDL-cholesterol, LDL-cholesterol, triglycerides, and total cholesterol to HDL ratio among subjects treated with Tenofovir Alafenamide and TDF in Trials 108 and 110 are presented in Table 8. (See Table 8).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn the open-label phase, lipid parameters at Week 120 in subjects who remained on Tenofovir Alafenamide were similar to those at Week 96. In subjects who switched from TDF to Tenofovir Alafenamide, mean change from Week 96 to Week 120 in total cholesterol was 23 mg/dL, HDL-cholesterol was 5 mg/dL, LDL-cholesterol was 16 mg/dL, triglycerides was 30 mg/dL, and total cholesterol to HDL ratio was 0 mg/dL.
Adverse Reactions in Virologically Suppressed Adult Subjects with Chronic Hepatitis B: The safety of Tenofovir Alafenamide in virologically suppressed adults is based on Week 48 data from a randomized, double-blind, active-controlled trial (Trial 4018) in which subjects taking TDF at baseline were randomized to switch to Tenofovir Alafenamide (N=243) or to continue their TDF treatment (N=245). Adverse reactions observed with Tenofovir Alafenamide in Trial 4018 were similar to those in Trials 108 and 110.
Renal Laboratory Tests, Bone Mineral Density Effects, and Serum Lipids: In virologically suppressed adults in Trial 4018, changes from baseline in renal function, BMD, and lipid parameters in the Tenofovir Alafenamide and TDF groups at Week 48 were similar to those observed in Trials 108 and 110 at Week 96.
Adverse Reactions in Adult Subjects with Chronic Hepatitis B and Renal Impairment: In an open-label trial (Trial 4035) in virologically suppressed adult subjects with chronic hepatitis B switching to Tenofovir Alafenamide 25 mg, the safety of Tenofovir Alafenamide was assessed in 78 subjects with moderate to severe renal impairment (estimated creatinine clearance between 15 and 59 mL per minute by Cockcroft-Gault method; Part A, Cohort 1) and 15 subjects with ESRD (estimated creatinine clearance below 15 mL per minute) receiving chronic hemodialysis (Part A, Cohort 2). The safety of Tenofovir Alafenamide, including changes from baseline in renal function, BMD, and lipid parameters, was similar to that observed in clinical trials of Tenofovir Alafenamide in subjects with compensated liver disease but without renal impairment (see Precautions).
Post marketing Experience: The following adverse reactions have been identified during post approval use of Tenofovir Alafenamide or other products containing tenofovir alafenamide. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Skin and Subcutaneous Tissue Disorders: Angioedema, urticaria.
Renal and Urinary Disorders: Acute renal failure, acute tubular necrosis, proximal renal tubulopathy, and Fanconi syndrome.
View ADR Monitoring Form