Clinical Trials Experience: Because clinical studies are conducted under widely varying conditions, adverse reaction rates observed in the clinical studies of a drug cannot be directly compared to rates in the clinical studies of another drug and may not reflect the rates observed in practice.
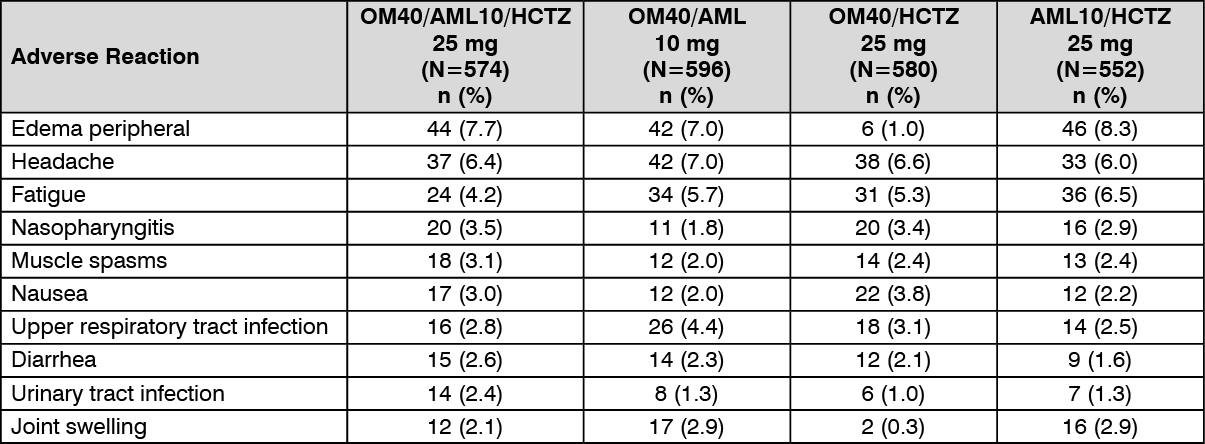
In the controlled trial of the combination of olmesartan, amlodipine & hydrochlorothiazide patients were randomized to this combination. Subjects who received triple combination therapy were treated between two and four weeks with one of the three dual combination therapies. Safety data from this study were obtained in 574 patients with hypertension who received this combination for 8 weeks.
The most common reason for discontinuation with this combination was dizziness (1%).
Dizziness was one of the most frequently reported adverse reactions with incidence of 1.4% to 3.6% in subjects continuing on dual combination therapy compared to 5.8% to 8.9% in subjects who switched to this combination.
The other most frequent adverse reactions that occurred in at least 2% of subjects are presented in the table as follows: (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Olmesartan medoxomil: Olmesartan medoxomil has been evaluated for safety in more than 3825 patients/subjects, including more than 3275 patients treated for hypertension in controlled trials. This experience included about 900 patients treated for at least 6 months and more than 525 treated for at least 1 year. Treatment with olmesartan medoxomil was well tolerated, with an incidence of adverse reactions similar to that seen with placebo. Adverse reactions were generally mild, transient, and without relationship to the dose of olmesartan medoxomil.
Amlodipine: Amlodipine has been evaluated for safety in more than 11,000 patients in clinical trials.
The following adverse reactions occurred in <1% but >0.1% of patients in controlled clinical trials under conditions of open trials or marketing experience where a causal relationship is uncertain; they are listed to alert physicians to a possible relationship:
Cardiovascular: arrhythmia (including ventricular tachycardia and atrial fibrillation), bradycardia, chest pain, hypotension, peripheral ischemia, syncope, tachycardia, postural dizziness, postural hypotension, vasculitis.
Central and Peripheral Nervous System: hypoesthesia, neuropathy peripheral, paresthesia, tremor, vertigo.
Gastrointestinal: anorexia, constipation, dyspepsia*, dysphagia, diarrhea, flatulence, pancreatitis, vomiting, gingival hyperplasia.
General: allergic reaction, asthenia*, back pain, hot flushes, malaise, pain, rigors, weight gain, weight decrease.
Musculoskeletal System: arthralgia, arthrosis, muscle cramps*, myalgia.
Psychiatric: sexual dysfunction (male* and female), insomnia, nervousness, depression, abnormal dreams, anxiety, depersonalization.
Respiratory: dyspnea*, epistaxis.
Skin and Appendages: angioedema, erythema multiforme, pruritus*, rash*, rash erythematous, rash maculopapular.
Special Senses: abnormal vision, conjunctivitis, diplopia, eye pain, tinnitus.
Urinary System: micturition frequency, micturition disorder, nocturia.
Autonomic Nervous System: dry mouth, sweating increased.
Metabolic and Nutritional: hyperglycemia, thirst.
Hemopoietic: leukopenia, purpura, thrombocytopenia.
* = events that occurred in less than 1% in placebo-controlled trials, but the incidence of these side effects was between 1% and 2% in all multiple dose studies.
The following adverse reactions occurred in <0.1% of patients: cardiac failure, pulse irregularity, extra systoles, skin discoloration, urticaria, skin dryness, alopecia, dermatitis, muscle weakness, twitching, ataxia, hypertonia, migraine, cold and clammy skin, apathy, agitation, amnesia, gastritis, increased appetite, loose stools, coughing, rhinitis, dysuria, polyuria, parosmia, taste perversion, abnormal visual accommodation, and xerophthalmia. Hydrochlorothiazide: Other adverse reactions that have been reported with hydrochlorothiazide, without regard to causality, are listed as follows:
Body as a Whole: weakness.
Digestive: pancreatitis, jaundice (intrahepatic cholestatic jaundice), sialadenitis, cramping, gastric irritation.
Hematologic: aplastic anemia, agranulocytosis, leukopenia, hemolytic anemia, thrombocytopenia.
Hypersensitivity: purpura, photosensitivity, urticaria, necrotizing angiitis (vasculitis and cutaneous vasculitis), fever, respiratory distress including pneumonitis and pulmonary edema, anaphylactic reactions.
Metabolic: hyperglycemia, glycosuria, hyperuricemia.
Musculoskeletal: muscle spasm.
Nervous System/Psychiatric: restlessness.
Renal: renal failure, renal dysfunction, interstitial nephritis.
Skin: erythema multiforme including Stevens-Johnson syndrome, exfoliative dermatitis including toxic epidermal necrolysis.
Special Senses: transient blurred vision, xanthopsia.
Post-Marketing Experience: The following adverse reactions have been identified during post-approval use of the individual components of Tri-Alzor. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Olmesartan medoxomil: The following adverse reactions have been reported in post-marketing experience:
Body as a Whole: asthenia, angioedema, anaphylactic reactions, peripheral edema.
Gastrointestinal: vomiting, diarrhea, sprue-like enteropathy.
Metabolic and Nutritional Disorders: hyperkalemia.
Musculoskeletal: rhabdomyolysis.
Urogenital System: acute renal failure, increased blood creatinine.
Skin and Appendages: alopecia, pruritus, urticaria.
Amlodipine: The following post-marketing event has been reported infrequently where a causal relationship is uncertain: gynecomastia. In post-marketing experience, jaundice and hepatic enzyme elevations (mostly consistent with cholestasis or hepatitis), in some cases severe enough to require hospitalization, have been reported in association with use of amlodipine. Post-marketing reporting has also revealed a possible association between extrapyramidal disorder and amlodipine.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out