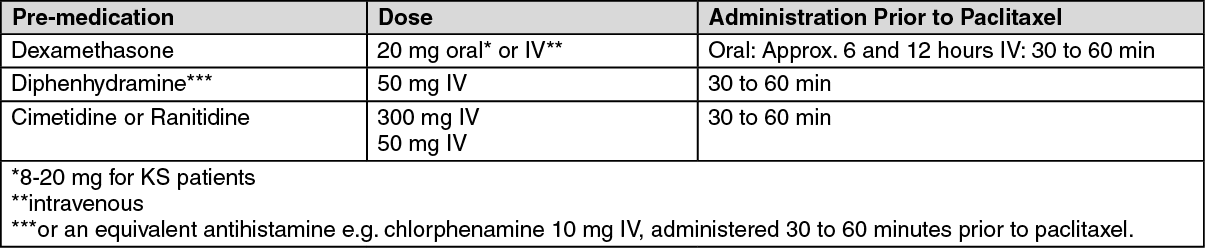
See table.
 Click on icon to see table/diagram/image
First-line treatment of ovarian cancer:
Click on icon to see table/diagram/image
First-line treatment of ovarian cancer: Although alternative medication regimens for paclitaxel are under investigation at present, a combination therapy of paclitaxel and cisplatin is recommended.
Depending on the duration of infusion, two different dosages are recommended for paclitaxel treatment: 175 mg/m
2 of paclitaxel is administered as an intravenous infusion over a period of three hours followed thereafter by 75 mg/m
2 of cisplatin and the therapy is repeated at 3-week intervals, or 135 mg/m
2 of paclitaxel is administered as an intravenous infusion over a period of 24 hours followed thereafter by 75 mg/m
2 of cisplatin and the therapy is repeated at 3-week intervals.
Second-line treatment of ovarian cancer: The recommended dose of paclitaxel is 175 mg/m
2 administered over 3 hours, with a 3-week interval between courses.
Adjuvant chemotherapy in breast carcinoma: The recommended dose of paclitaxel is 175 mg/m
2 administered over a period of 3 hours every 3 weeks for four courses, following AC therapy.
First-line chemotherapy of breast carcinoma: When used in combination with doxorubicin (50 mg/m
2), paclitaxel should be administered 24 hours after doxorubicin. The recommended dose of paclitaxel is 220 mg/m
2 administered intravenously over a period of 3 hours, with a 3-week interval between courses.
When used in combination with trastuzumab, the recommended dose of paclitaxel is 175 mg/m
2 administered intravenously over a period of 3 hours, with a 3-week interval between courses. Paclitaxel infusion may be started the day following the first dose of trastuzumab or immediately after the subsequent doses of trastuzumab if the preceding dose of trastuzumab was well tolerated.
Second-line chemotherapy of breast carcinoma: The recommended dose of paclitaxel is 175 mg/m
2 administered intravenously over a period of 3 hours, with a 3-week interval between courses.
Advanced non-small cell lung cancer: The recommended dose of paclitaxel is 175 mg/m
2 administered over 3 hours followed by 80 mg/m
2 of cisplatin, with a 3-week interval between courses.
Treatment of AIDS-related KS: The recommended dose of paclitaxel is 100 mg/m
2 administered as a 3 hour intravenous infusion every two weeks.
Dose adjustment: Subsequent doses of paclitaxel should be administered according to individual patient tolerance. Paclitaxel should not be re-administered until the neutrophil count is ≥1.5 x 10
9/L (≥1 x 10
9/L for KS patients) and the platelet count is ≥100 x 10
9/L (≥75 x 10
9/L for KS patients).
Patients, who experience severe neutropenia (neutrophil count <0.5 x 10
9/L for a minimum of 7 days) or severe peripheral neuropathy, should receive a dose reduction of 20% for subsequent courses (25% for KS patients).
Patients with hepatic impairment: Inadequate data are available to recommend dosage alterations in patients with mild to moderate hepatic impairment. Paclitaxel is not recommended in patients with severely impaired hepatic function.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagec3d63b82-208c-4071-b898-a7e40147bc41.GIF)
ab927889-33ce-478c-aa79-a7e40147bc32.GIF)
4cc1d99c-b3c8-4e2d-9b86-a7e40147bc4f.GIF)

 Sign Out
Sign Out