Pharmacology: Mechanism of action: Increased levels of signaling through the vascular endothelial growth factor A (VEGF-A) pathway are associated with pathologic ocular angiogenesis and retinal edema. Brolucizumab binds with high affinity to VEGF-A isoforms (e.g. VEGF
110, VEGF
121, and VEGF
165), thereby preventing binding of VEGF-A to its receptors VEGFR-1 and VEGFR-2. By inhibiting VEGF-A binding, brolucizumab suppresses endothelial cell proliferation, thereby reducing pathologic neovascularization and decreasing vascular permeability.
Pharmacodynamics: Wet AMD: In the HAWK and HARRIER studies, related anatomical parameters were part of the disease activity assessments guiding treatment decisions. Reductions in central subfield thickness (CST) and in presence of intraretinal/subretinal fluid (IRF/SRF) or sub-retinal pigment epithelium (sub-RPE) fluid were observed in patients treated with Brolucizumab (Vsiqq) as early as 4 weeks after treatment initiation and up to Week 48 and Week 96. Statistically significant greater reductions in CST and in presence of IRF/SRF relative to aflibercept were demonstrated at Weeks 16 and 48 (see CLINICAL STUDIES as follows).
In these studies, for patients treated with Brolucizumab (Vsiqq), reductions in CNV lesion size were observed as early as 12 weeks, and at Weeks 48 and 96, after treatment initiation.
DME: In the KESTREL and KITE studies, related anatomical parameters were part of the disease activity assessments guiding treatment decisions. Reductions in central subfield thickness (CST) and in presence of intraretinal/subretinal fluid (IRF/SRF) were observed in patients treated with Brolucizumab (Vsiqq) as early as 4 weeks after treatment initiation and up to Week 52.
Clinical Studies: Treatment of wet AMD: The safety and efficacy of Brolucizumab (Vsiqq) were assessed in two randomized, multicenter, double-masked, active-controlled Phase III studies (HAWK and HARRIER) in patients with neovascular (wet) AMD. A total of 1,817 patients were treated in these studies for two years (1,088 on Brolucizumab (Vsiqq) and 729 on aflibercept). Patient ages ranged from 50 to 97 years with a mean age of 76 years.
In HAWK, patients were randomized in a 1:1:1 ratio to the following dosing regimens: brolucizumab 3 mg administered every 12 or 8 weeks (q12w/q8w) after the first 3 monthly doses; brolucizumab 6 mg administered every 12 or 8 weeks (q12w/q8w) after the first 3 monthly doses; aflibercept 2 mg administered every 8 weeks (q8w) after the first 3 monthly doses.
In HARRIER, patients were randomized in a 1:1 ratio to the following dosing regimens: brolucizumab 6 mg administered every 12 or 8 weeks (q12w/q8w) after the first 3 monthly doses; aflibercept 2 mg administered every 8 weeks (q8w) after the first 3 monthly doses.
In both studies, after the first three monthly doses (Week 0, 4 and 8), brolucizumab patients were treated q12w, with the option of adjusting to q8w dosing interval based on disease activity. Disease activity was assessed by a physician during the first q12 week interval (at Week 16 and 20) and at each subsequent scheduled q12w treatment visit. Patients who showed disease activity (e.g. decreased visual acuity, increased central subfield thickness (CST), and/or presence of retinal fluids (IRF/SRF, sub-RPE)) at any of these visits were adjusted to a q8w treatment interval.
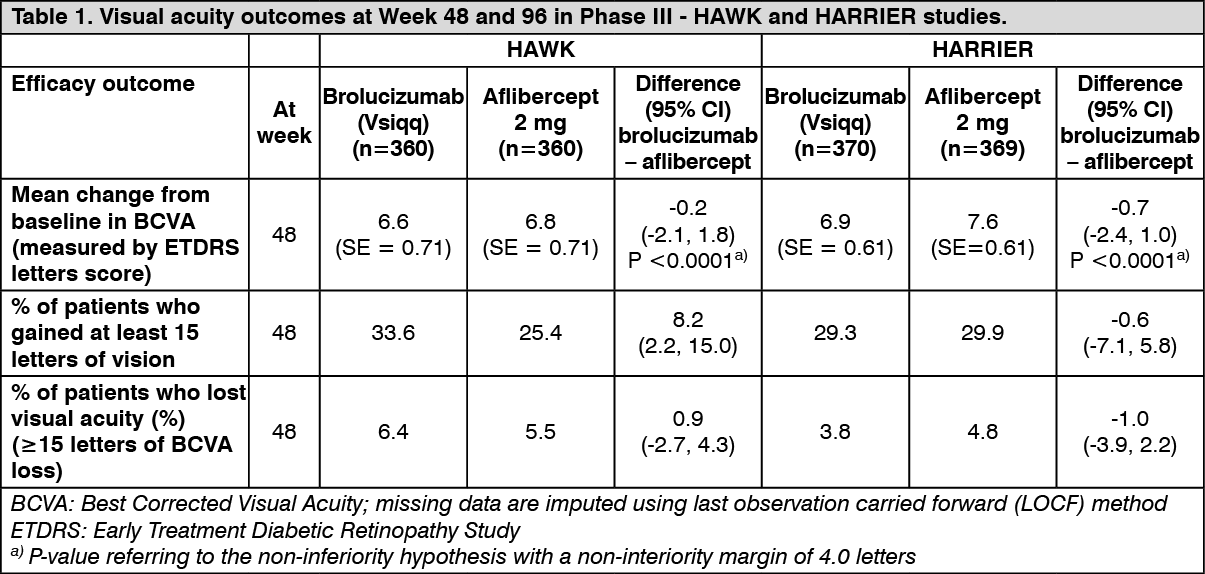
Results: The primary efficacy endpoint for the studies was the change from baseline in Best Corrected Visual Acuity (BCVA) to Week 48 as measured by the Early Treatment Diabetic Retinopathy Study (ETDRS) Letter Score with the primary objective to demonstrate non-inferiority of Brolucizumab (Vsiqq) vs. aflibercept. In both studies, Brolucizumab (Vsiqq) (administered in a q12w/q8w regimen) demonstrated non-inferior efficacy to aflibercept 2 mg (administered q8w). The visual acuity gains observed in the first year were maintained in the second year.
Detailed results of both studies are shown in Table 1 and Figure 1 as follows. (See Table 1 and Figure 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
These visual acuity gains were achieved with 56% and 51% patients treated with Brolucizumab (Vsiqq) on q12w dosing interval at Week 48, and with 45% and 39% of patients at Week 96 in HAWK and HARRIER, respectively. Among patients identified as eligible for q12w interval during the first 12 week interval, 85% and 82% remained on the q12w dosing interval up to Week 48. Of patients on the q12w interval at Week 48, 82% and 75% remained on the 12 week dosing interval through Week 96.
Treatment effects in evaluable subgroups (e.g., age, gender, race, baseline visual acuity, baseline retinal thickness, lesion type, lesion size, fluid status) in each study were generally consistent with the results in the overall population.
Disease activity was assessed by changes in visual acuity and/or anatomical parameters, including central subfield thickness (CST) and/or presence of retinal fluids (IRF/SRF, sub-RPE). At Week 16, when disease activity was first assessed for determining the treatment interval, statistically fewer patients showed disease activity on Brolucizumab (Vsiqq) compared to aflibercept 2 mg. Disease activity was assessed throughout the studies. Anatomical parameters of disease activity were decreased at Week 48 for Brolucizumab (Vsiqq) compared to aflibercept (Table 2). (See Table 2.)
Click on icon to see table/diagram/image
In both studies, Brolucizumab (Vsiqq) demonstrated clinically meaningful increases from baseline in the pre-specified secondary efficacy endpoint of patient reported outcomes, reported through the National Eye Institute Visual Function Questionnaire (NEI VFQ-25). The magnitude of these changes was similar to that seen in published studies, which corresponded to a 15-letter gain in Best Corrected Visual Acuity (BCVA). Patient reported outcomes benefits were maintained in the second year.
No clinically meaningful differences were found between Brolucizumab (Vsiqq) and aflibercept in changes from baseline to Week 48 in NEI VFQ-25 total score and subscales (general vision, ocular pain, near activities, distance activities, social functioning, mental health, role difficulties, dependency, driving, color vision, and peripheral vision).
Treatment of DME: The safety and efficacy of Brolucizumab (Vsiqq) were assessed in two randomized, multicenter, double-masked, active controlled, Phase III studies (KESTREL and KITE) in patients with diabetic macular edema (DME).
A total of 926 patients were treated in these studies for 1 year (558 on brolucizumab and 368 on aflibercept 2 mg). Patient ages ranged from 23 to 87 years with a mean of 63 years.
In KESTREL, patients were randomized in a 1:1:1 ratio to the following dosing regimens: brolucizumab 6 mg administered once every 6 weeks (q6w) for first 5 doses, followed by brolucizumab 6 mg every 12 or 8 weeks (q12w/q8w).
Brolucizumab 3 mg administered once every 6 weeks (q6w) for first 5 doses, followed by brolucizumab 3 mg every 12 or 8 weeks (q12w/q8w).
Aflibercept 2 mg administered once every 4 weeks (q4w) for first 5 doses, followed by aflibercept 2 mg every 8 weeks (q8w).
In KITE, patients were randomized in a 1:1 ratio to the following dosing regimens: brolucizumab 6 mg administered once every 6 weeks (q6w) for first 5 doses, followed by brolucizumab 6 mg every 12 or 8 weeks (q12w/q8w).
Aflibercept 2 mg administered once every 4 weeks (q4w) for first 5 doses, followed by aflibercept 2 mg every 8 weeks (q8w).
In both studies, after the first five doses (Weeks 0, 6, 12, 18 and 24), brolucizumab patients were treated q12w, with the option of adjusting to a q8w dosing interval based on disease activity. Disease activity was assessed by a physician during the first q12 week interval (at Weeks 32 and 36) and at each subsequent scheduled q12w treatment visit. Patients who showed disease activity (e.g. decreased visual acuity, increased central subfield thickness) at any of these visits were adjusted to a q8w treatment interval. The comparator aflibercept was administered every 8 weeks after the first 5 monthly doses.
Results: The primary efficacy endpoint for both studies was the change from baseline at Week 52 in Best Corrected Visual Acuity (BCVA) as measured by the Early Treatment Diabetic Retinopathy Study (ETDRS) Letter Score with the primary objective to demonstrate noninferiority of Brolucizumab (Vsiqq) versus aflibercept 2 mg. In both studies, Brolucizumab (Vsiqq) (administered in a q12w/q8w regimen) demonstrated non-inferior efficacy to aflibercept 2 mg (administered q8w).
The results of KESTREL and KITE also demonstrated non-inferiority of Brolucizumab (Vsiqq) versus aflibercept 2 mg for the key secondary endpoint (average change from baseline in BCVA over the period Week 40 through Week 52).
The median number of injections given over 12 months was 7 in patients treated with Brolucizumab (Vsiqq) versus 9 in patients treated with aflibercept 2 mg.
Detailed results of both studies are shown in Table 3 and Figure 2 as follows. (See Table 3 and Figure 2.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
These visual acuity gains were achieved with 55% and 50% of patients treated with Brolucizumab (Vsiqq) on a q12w dosing interval at Week 52 in KESTREL and KITE, respectively. Among patients identified as eligible for q12w dosing during the first 12-week interval, 88% and 95% remained on the q12w dosing interval at Week 52.
Treatment effects in evaluable subgroups (i.e. age, gender, baseline HbA1c, baseline visual acuity, baseline central subfield thickness, DME lesion type, duration of DME since diagnosis, retinal fluid status) in each study were generally consistent with the results in the overall population.
Disease activity (DA) was assessed by changes in visual acuity and/or anatomical parameters, including CST and/or presence of IRF/SRF. Disease activity was assessed throughout the studies. At the first assessment at Week 32, disease activity was observed in 20.1% and 24.2% of patients treated with Brolucizumab (Vsiqq) (5 injections received) and 27.8% and 39.8% of patients treated with aflibercept 2 mg (6 injections received) in KESTREL and KITE, respectively.
In both studies, Brolucizumab (Vsiqq) demonstrated a significant reduction from baseline in CST starting at Week 4 and continuing up to Week 52. In KITE, the average reduction from baseline over the period Week 40 to Week 52 with Brolucizumab (Vsiqq) was statistically superior to that observed with aflibercept 2 mg. From Week 40 to Week 52, the proportion of patients with IRF/SRF was lower in patients treated with Brolucizumab (Vsiqq) (range 54% to 65%) compared to patients treated with aflibercept 2 mg (range 71% to 80%).
In both studies, Brolucizumab (Vsiqq) demonstrated increases from baseline in the prespecified secondary efficacy endpoint of patient reported outcomes, reported through the National Eye Institute Visual Function Questionnaire (NEI VFQ-25). The magnitude of these changes was similar to that seen in published studies, which corresponded to a 15-letter gain in Best Corrected Visual Acuity (BCVA).
No differences were found between Brolucizumab (Vsiqq) and aflibercept 2 mg in changes from baseline to Week 52 in NEI VFQ-25 total score and subscales (general vision, ocular
pain, near activities, distance activities, social functioning, mental health, role difficulties,
dependency, driving, color vision, and peripheral vision).
Diabetic retinopathy severity score (DRSS) was assessed in the KESTREL and KITE studies. At baseline, 98.1% of patients in both KESTREL and KITE had gradable DRSS scores. Based on the pooled analysis, 28.9% of patients treated with Brolucizumab (Vsiqq) experienced a ≥2 step improvement from baseline to Week 52 in the DRSS score compared to 24.9% of patients treated with aflibercept 2 mg. The estimated difference between Brolucizumab (Vsiqq) and aflibercept 2 mg was 4.0% (95% CI: [-0.6, 8.6]).
Pharmacokinetics: Brolucizumab (Vsiqq) is administered directly into the vitreous to exert local effects in the eye.
Absorption/Distribution: After intravitreal administration of 6 mg brolucizumab per eye to patients with nAMD, the mean C
max of free brolucizumab in the plasma was 49.0 ng/mL (range: 8.97 to 548 ng/mL) and was attained in 1 day.
Metabolism/Elimination: Brolucizumab is a monoclonal antibody fragment and no drug metabolism studies have been conducted. As a single-chain antibody fragment, free brolucizumab is expected to undergo elimination through both target-mediated disposition via binding to free endogenous VEGF, passive renal elimination, and metabolism via proteolysis.
After intravitreal injections, brolucizumab was eliminated with an apparent systemic half-life of 4.4 days. Concentrations were generally near or below the quantitation limit (<0.5 ng/mL) approximately 4 weeks after dosing in most patients. Brolucizumab (Vsiqq) did not accumulate in the serum when administered intravitreally every 4 weeks.
Special populations: Geriatric patients (65 years or above): In the HAWK and HARRIER clinical studies, approximately 90% (978/1088) of patients randomized to treatment with Brolucizumab (Vsiqq) were ≥65 years of age and approximately 60% (648/1088) were ≥75 years of age. In the KESTREL and KITE clinical studies, approximately 45% (164/368) of patients randomized to treatment with Brolucizumab (Vsiqq) were ≥ 65 years of age and approximately 10% (37/368) were ≥ 75 years of age. No significant differences in efficacy or safety were seen with increasing age in these studies.
Race/Ethnicity: There were no ethnic differences in systemic pharmacokinetics following intravitreal injection in a study with 24 Caucasian and 26 Japanese patients.
Renal impairment: Mild to severe renal impairment should have no impact on the overall systemic exposure to brolucizumab, because the systemic concentration of brolucizumab is driven by the distribution from the eye rather than the elimination rate and because the systemic exposure of free brolucizumab is low.
The systemic clearance of brolucizumab was evaluated in nAMD patients who had both serum brolucizumab pharmacokinetic and creatinine clearance data available. Subjects with mild (50 to 79 mL/min (n=13)) renal impairment had mean systemic clearance rates of brolucizumab which were within 15% of the mean clearance rate for subjects with normal renal function (≥80 mL/min (n=25)). Patients with moderate (30 to 49 mL/min (n=3)) renal impairment had mean systemic clearance rates of brolucizumab which were lower than patients with normal renal function but the number of patients was too low to make definitive conclusions. No patients with severe (<30 mL/min) renal impairment were studied.
Hepatic impairment: Mild to severe hepatic impairment should have no impact on the overall systemic exposure to brolucizumab, because metabolism occurs via proteolysis and does not depend on hepatic function.
Toxicology: Non-Clinical Safety Data: Carcinogenicity and mutagenicity: No studies have been conducted on the carcinogenic or mutagenic potential of Brolucizumab (Vsiqq).
Repeat dose toxicity: Non-clinical data reveal no special hazard for humans based on 3- and 6-month repeated dose toxicity studies. Intravitreal injections of brolucizumab to cynomolgus monkeys at doses up to 6 mg per eye every 4 weeks for 26 weeks resulted in no ocular or systemic effects and were well-tolerated.
Evaluations included daily observations for morbidity and mortality, clinical observations (including abnormal respiration and behavior), body weight determinations, biomicroscopic and indirect ophthalmoscopic examinations, intraocular pressure measurements, electroretinograms, clinical pathology, toxicokinetic and anti-drug antibody analysis of the serum and vitreous, and macroscopic and microscopic examinations.
The ocular and systemic no observed adverse effect level (NOAEL) with brolucizumab 6 mg per eye every 4 weeks provides a 2-fold margin of ocular safety (based on comparative ocular volume) for the recommended human dose.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image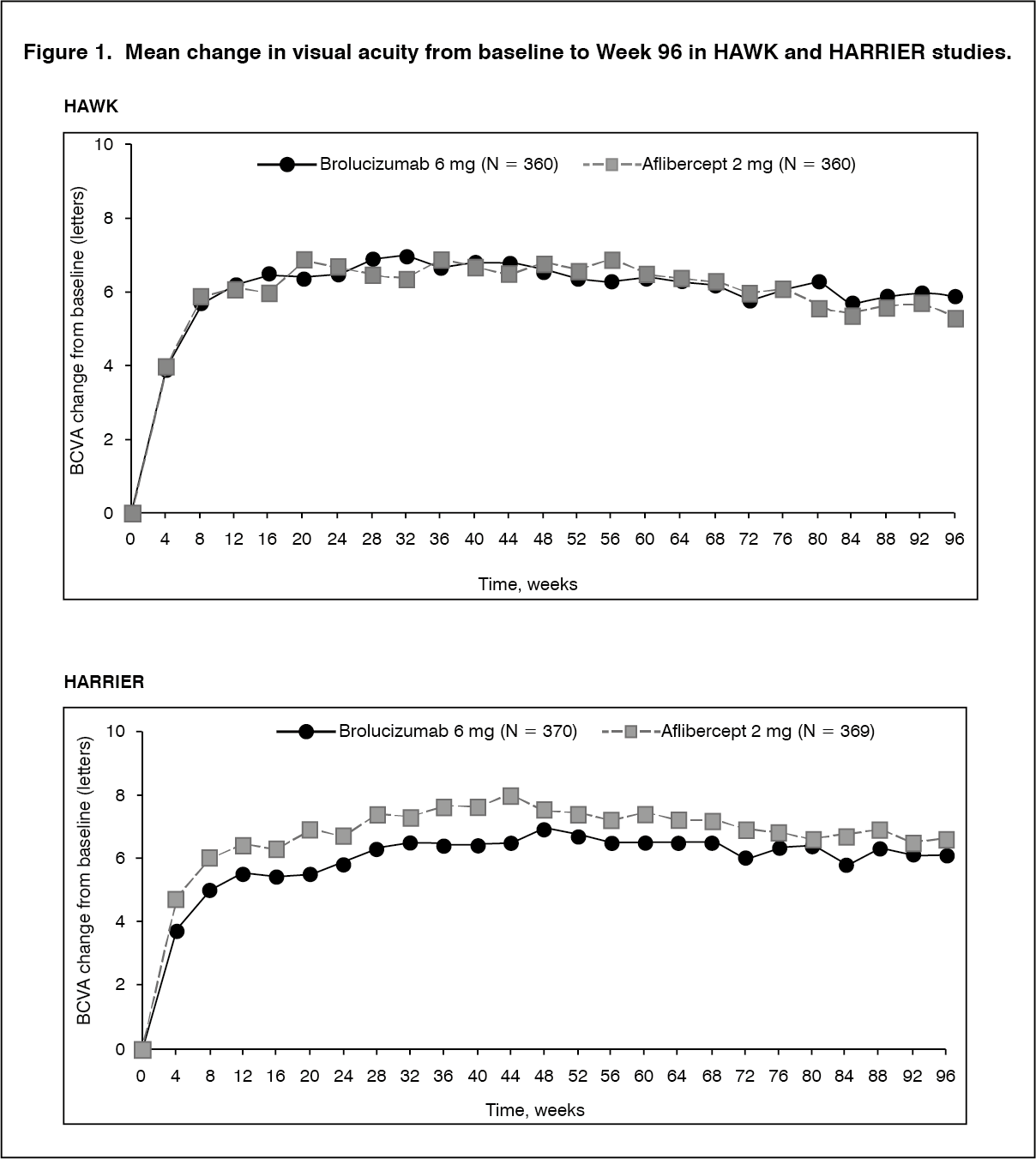 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image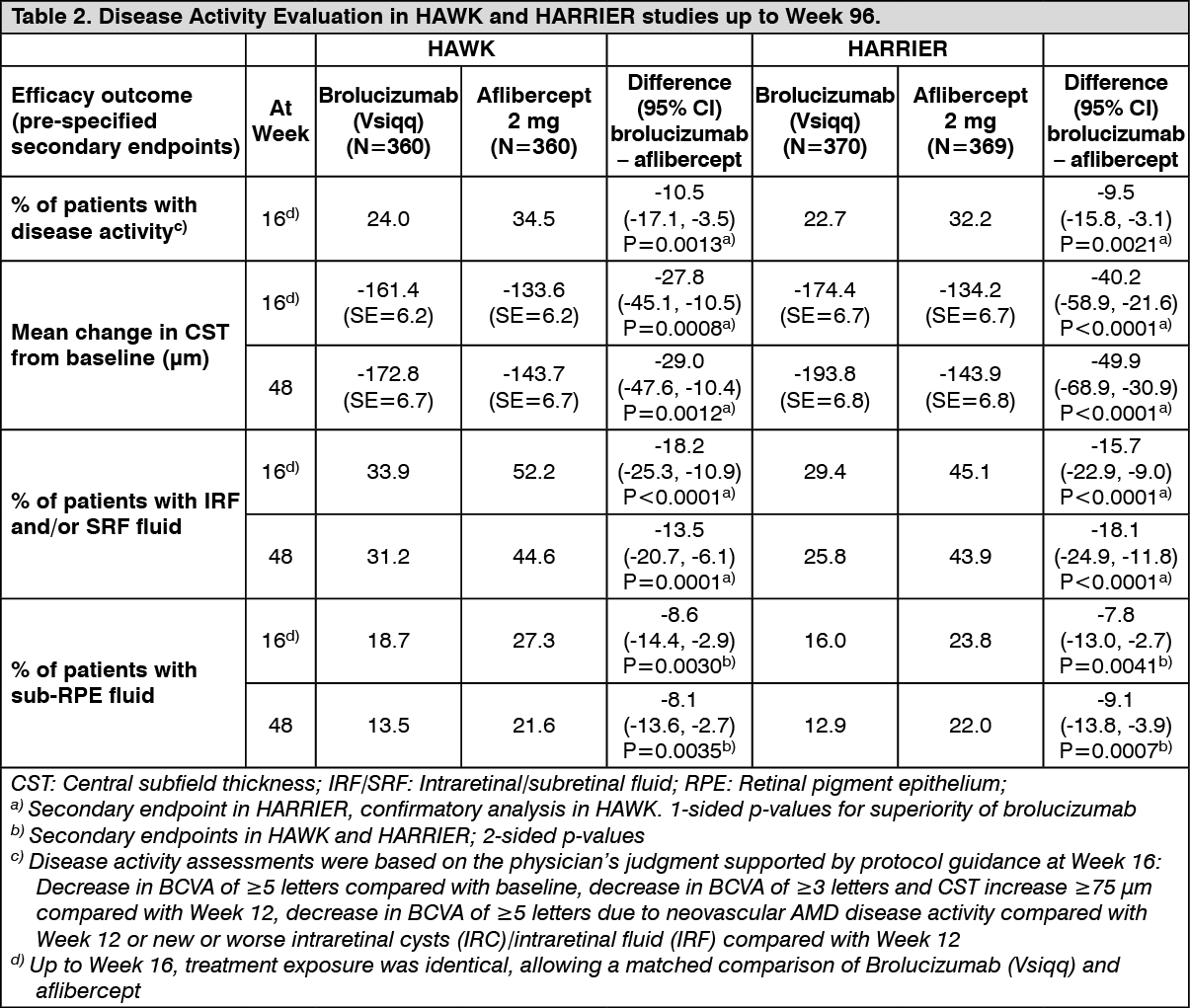 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image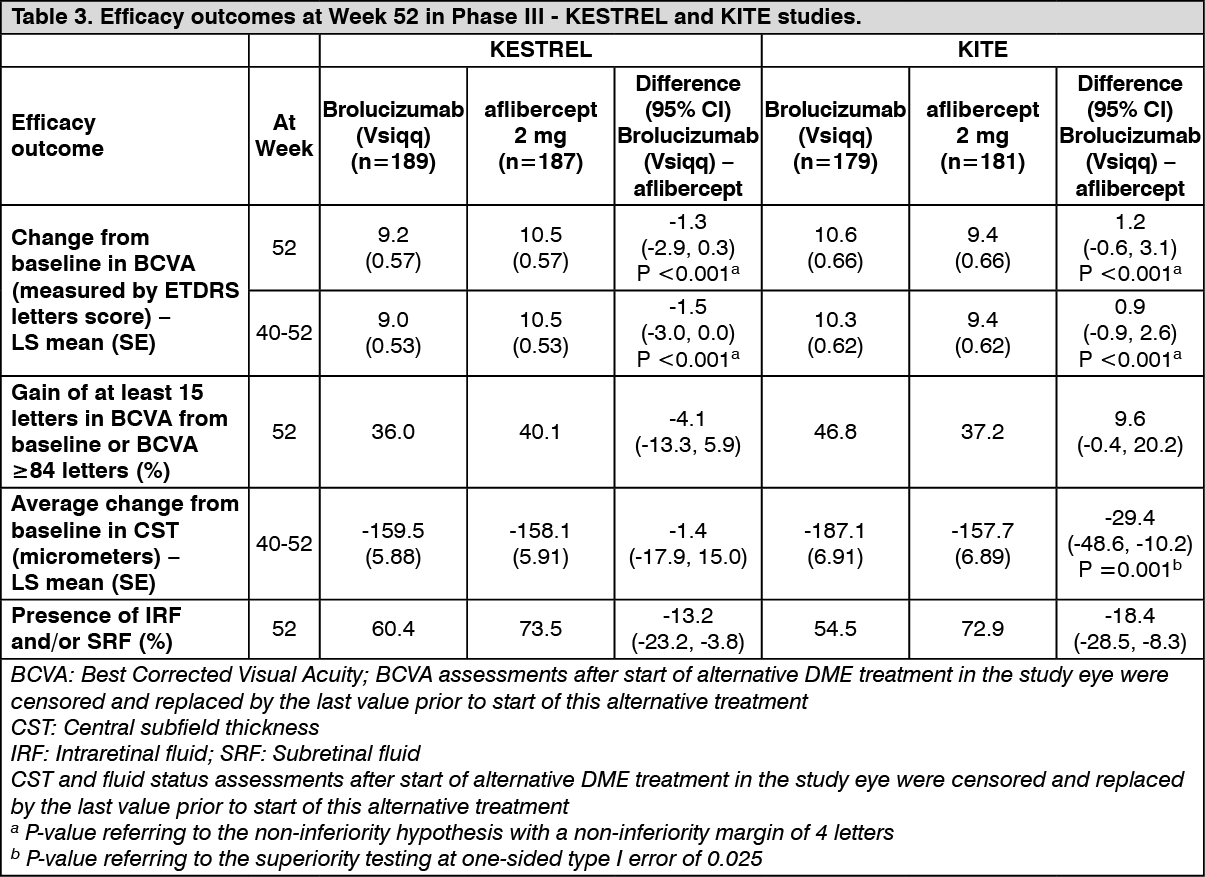 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image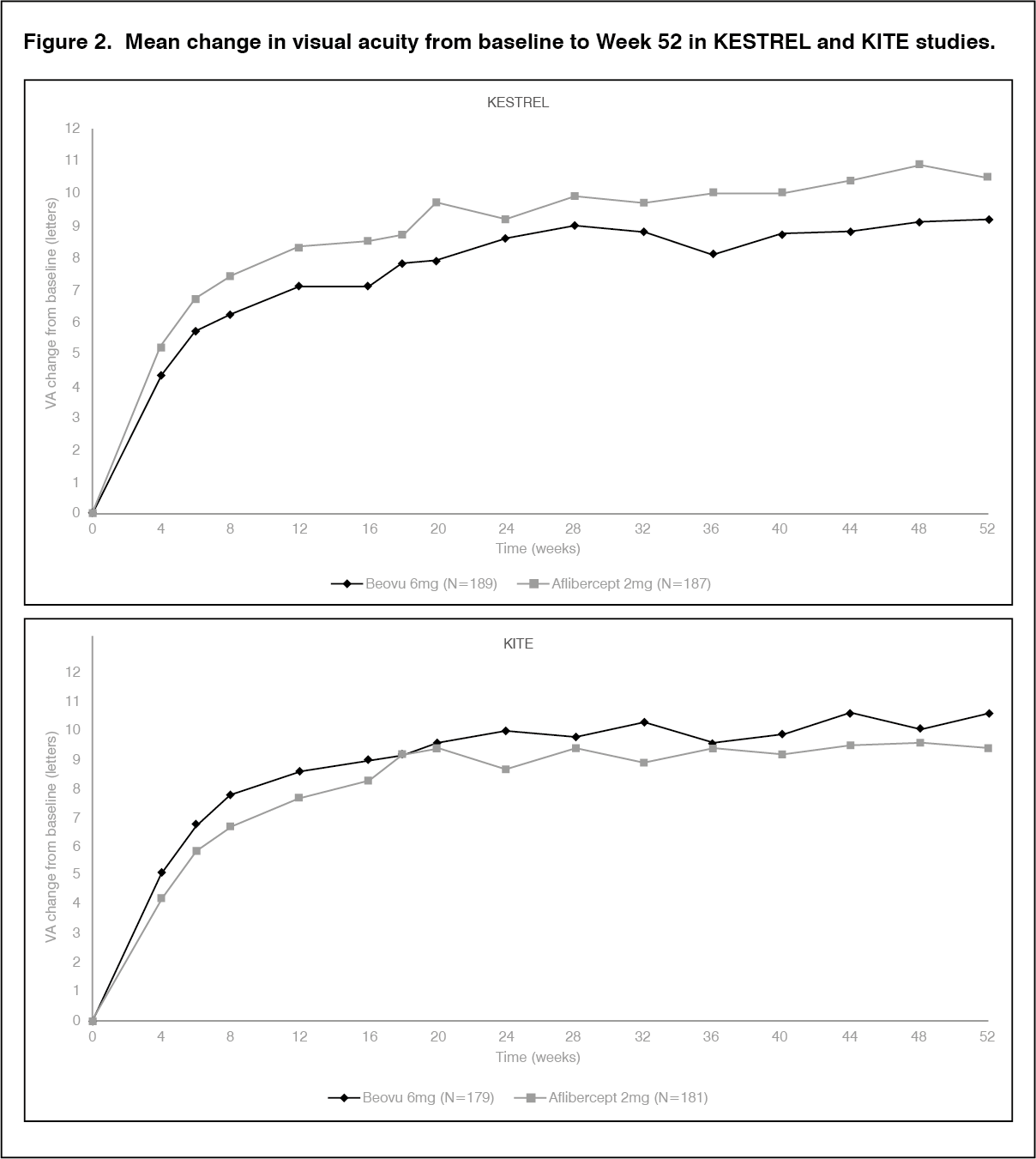 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out