


 Sign Out
Sign Out
Pharmacology: Pharmacodynamics: Human G-CSF is a glycoprotein which regulates the production and release of functional neutrophils from the bone marrow. Filgrastim Solution for Injection containing r-metHuG-CSF (filgrastim) causes marked increases in peripheral blood neutrophil counts within 24 hours, with minor increases in monocytes. In some SCN patients, filgrastim can also induce a minor increase in the number of circulating eosinophils and basophils relative to baseline; some of these patients may present with eosinophilia or basophilia already prior to treatment.
Elevations of neutrophil counts are dose-dependent at recommended doses. Neutrophils produced in response to filgrastim show normal or enhanced function as demonstrated by tests of chemotactic and phagocytic function. Following termination of filgrastim therapy, circulating neutrophil counts decrease by 50% within 1-2 days, and to normal levels within 1-7 days.
Use of filgrastim in patients undergoing cytotoxic chemotherapy leads to significant reductions in the incidence, severity and duration of neutropenia and febrile neutropenia. Treatment with filgrastim significantly reduces the duration of febrile neutropenia, antibiotic use and hospitalisation after induction chemotherapy for acute myelogenous leukaemia or myeloablative therapy followed by bone marrow transplantation. The incidence of fever and documented infections were not reduced in either setting. The duration of fever was not reduced in patients undergoing myeloablative therapy followed by bone marrow transplantation.
Use of filgrastim, either alone, or alter chemotherapy, mobilises haematopoietic progenitor cells into the peripheral blood. These autologous PBPCs may be harvested and infused alter high-dose cytotoxic therapy, either in place of, or in addition to bone marrow transplantation. Infusion of PBPC accelerates haematopoietic recovery reducing the duration of risk for haemorrhagic complications and the need for platelet transfusions.
Recipients of allogeneic PBPCs mobilised with filgrastim experienced significantly more rapid haematological recovery, leading to a significant decrease in time to unsupported platelet recovery when compared with allogeneic bone marrow transplantation.
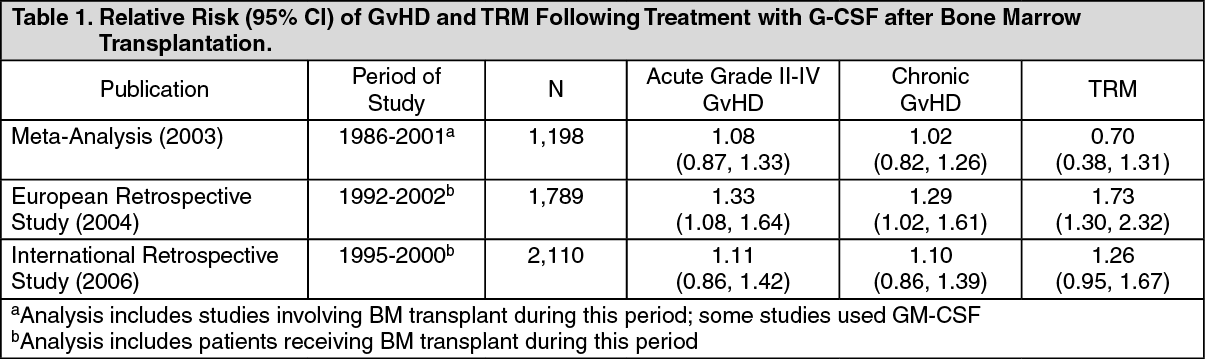
One retrospective European study evaluating the use of G-CSF alter allogeneic bone marrow transplantation in patients with acute leukaemias suggested an increase in the risk of GvHD, treatment related mortality (TRM) and mortality when G-CSF was administered. In a separate retrospective international study in patients with acute and chronic myelogenous leukaemias, no effect on the risk of GvHD, TRM and mortality was seen. A meta-analysis of allogeneic transplant studies, including the results of nine prospective randomised trials, eight retrospective studies and one case-controlled study, did not detect an effect on the risks of acute GvHD, chronic GvHD or early treatment-related mortality. See Table 1.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageUse of filgrastim for the mobilisation of PBPCs in normal donors prior to allogeneic PBPC transplantation: In normal donors, a 1.0 MU/kg/day (10 μg/kg/day) dose administered subcutaneously for 4-5 consecutive days allows a collection of ≥4 x 106 CD34+ cells/kg recipient BW in the majority of the donors alter two leukaphereses.
Use of filgrastim in patients, children or adults, with SCN (severe congenital, cyclic, and idiopathic neutropenia) induces a sustained increase in ANCs in peripheral blood and a reduction of infection and related events.
Use of filgrastim in patients with HIV infection maintains normal neutrophil counts to allow scheduled dosing of antiviral and/or other myelosuppressive medication. There is no evidence that patients with HIV infection treated with filgrastim show an increase in HIV replication.
As with other haematopoietic growth factors, G-CSF has shown in vitro stimulating properties on human endothelial cells.
Pharmacokinetics: Randomised, double-blind, single and multiple dose, crossover studies in 204 healthy volunteers showed that the pharmacokinetic profile of filgrastim was comparable to that of the reference product after subcutaneous and intravenous administration.
Absorption: A single subcutaneous dose of 0.5 MU/kg (5 μg/kg) resulted in maximum serum concentrations after a tmax of 4.5 ± 0.9 hours (mean± SD).
Distribution: The volume of distribution in blood is approximately 150 mL/kg. Following subcutaneous administration of recommended doses, serum concentrations were maintained above 10 ng/mL for 8-16 hours. There is a positive linear correlation between the dose and the serum concentration of filgrastim, whether administered intravenously or subcutaneously.
Elimination: The median serum elimination half-life (t½) of filgrastim after single subcutaneous doses ranged from 2.7 hours ( 1.0 MU/kg, 10 μg/kg) to 5.7 hours (0.25 MU/kg, 2.5 μg/kg) and was prolonged after 7 days of dosing to 8 .5-14 hours, respectively.
Continuous infusion with filgrastim over a period of up to 28 days, in patients recovering from autologous bone-marrow transplantation, resulted in no evidence of active substance accumulation and comparable elimination half-lives.
Toxicology: Preclinical safety data: Filgrastim was studied in repeated dose toxicity studies up to 1 year in duration which revealed changes attributable to the expected pharmacological actions including increases in leukocytes, myeloid hyperplasia in bone marrow, extramedullary granulopoiesis and splenic enlargement. These changes all reversed after discontinuation of treatment.
Effects of filgrastim on prenatal development have been studied in rats and rabbits. Intravenous (80 μg/kg/day) administration of filgrastim to rabbits during the period of organogenesis was maternally toxic and increased spontaneous abortion, post-implantation loss, and decreased mean live litter size and foetal weight were observed.
Based on reported data for another filgrastim product similar to the reference filgrastim product, comparable findings plus increased foetal malformations were observed at 100 μg/kg/day, a maternally toxic dose which corresponded to a systemic exposure of approximately 50-90 times the exposures observed in patients treated with the clinical dose of 5 μg/kg/day. The observed adverse effect level for embryo-foetal toxicity in this study was 10 μg/kg/day, which corresponded to a systemic exposure of approximately 3-5 times the exposures observed in patients treated with the clinical dose.
In pregnant rats, no maternal or foetal toxicity was observed at doses up to 575 μg/kg/day. Offspring of rats administered filgrastim during the peri-natal and lactation periods, exhibited a delay in external differentiation and growth retardation (≥20 μg/kg/day) and slightly reduced survival rate (100 μg/kg/day).
Filgrastim had no observed effect on the fertility of male or female rats.