


 Sign Out
Sign Out
 Click on icon to see table/diagram/image
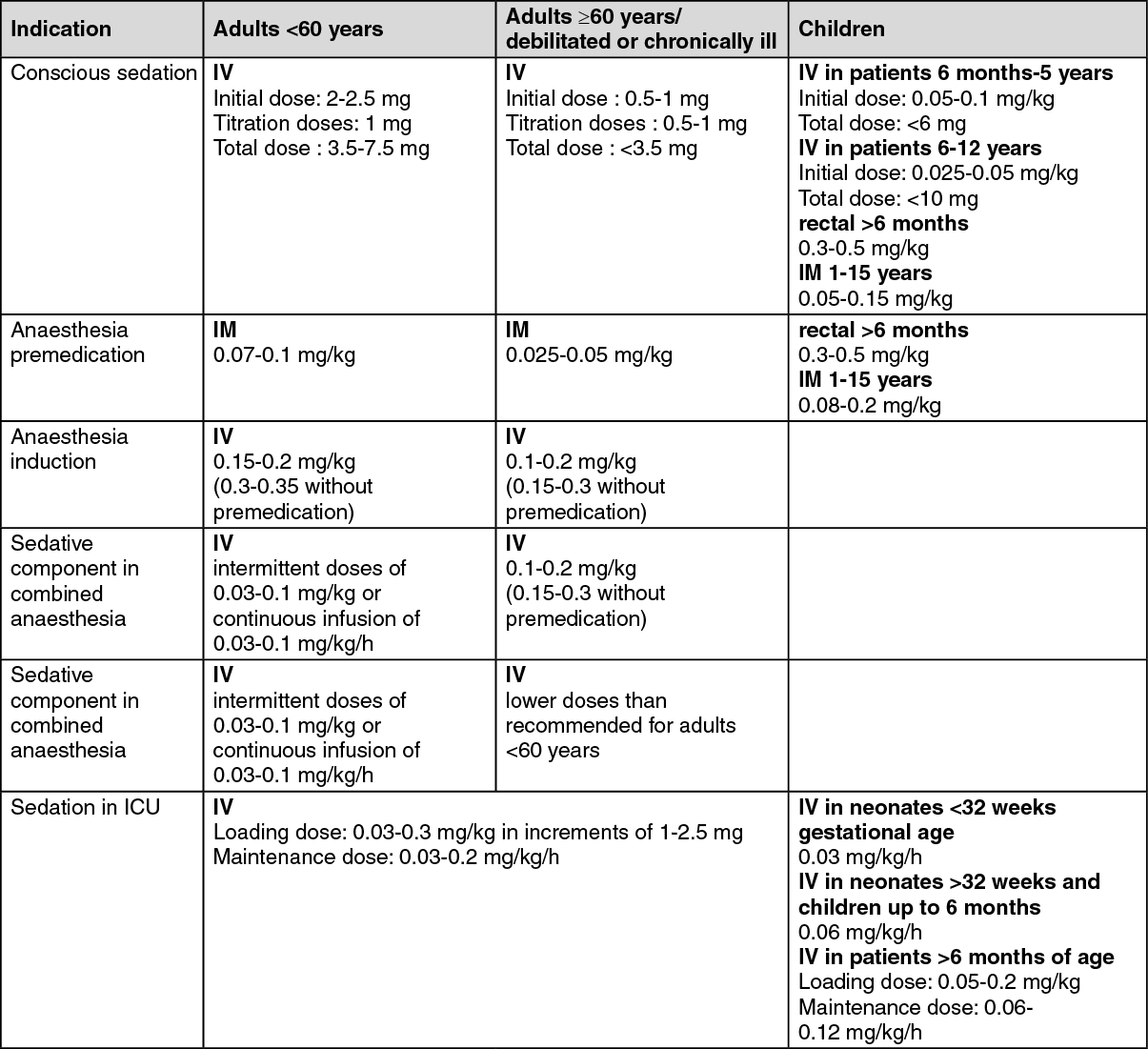
Click on icon to see table/diagram/imageCONSCIOUS SEDATION DOSAGE: For conscious sedation prior to diagnostic or surgical intervention, midazolam is administered IV. The dose must be individualised and titrated, and should not be administered by rapid or single bolus injection. The onset of sedation may vary individually depending on the physical status of the patient and the detailed circumstances of dosing (e.g. rate of administration, amount of dose). If necessary, subsequent doses may be administered according to the individual need. The onset of action is about 2 minutes after the injection. Maximum effect is obtained in about 5 to 10 minutes.
Adults: The IV injection of midazolam should be given slowly at a rate of approximately 1 mg in 30 seconds.
In adults below the age of 60 the initial dose is 2 to 2.5mg given 5 to 10 minutes before the beginning of the procedure. Further doses of 1mg may be given as necessary. Mean total doses have been found to range from 3.5 to 7.5mg. A total dose greater than 5mg is usually not necessary.
In adults over 60 years of age, debilitated or chronically ill patients, the initial dose must be reduced to 0.5-1.0mg and given 5-10 minutes before the beginning of the procedure. Further doses of 0.5 to 1 mg may be given as necessary.
Paediatric population: IV administration: midazolam should be titrated slowly to the desired clinical effect. The initial dose of midazolam should be administered over 2 to 3 minutes. One must wait an additional 2 to 5 minutes to fully evaluate the sedative effect before initiating a procedure or repeating a dose. If further sedation is necessary, continue to titrate with small increments until the appropriate level of sedation is achieved. Infants and young children less than 5 years of age may require substantially higher doses (mg/kg) than older children and adolescents.
Paediatric patients less than 6 months of age: paediatric patients less than 6 month of age are particularly vulnerable to airway obstruction and hypoventilation. For this reason, the use in conscious sedation in children less than 6 months of age is not recommended.
Paediatric patients 6 months to 5 years of age: initial dose 0.05 to 0.1mg/kg. A total dose up to 0.6mg/kg may be necessary to reach the desired endpoint, but the total dose should not exceed 6mg.
Prolonged sedation and risk of hypoventilation may be associated with the higher doses.
Paediatric patients 6 to 12 years of age: initial dose 0.025 to 0.05mg/kg. A total dose of up to 0.4mg/kg to a maximum of 10mg may be necessary. Prolonged sedation and risk of hypoventilation may be associated with the higher doses.
Paediatric patients 12 to 16 years of age: should be dosed as adults.
Rectal administration: the total dose of midazolam usually ranges from 0.3 to 0.5mg/kg. Rectal administration of the ampoule/vial solution is performed by means of a plastic applicator fixed on the end of the syringe. If the volume to be administered is too small, water may be added up to a total volume of 10ml. Total dose should be administered at once and repeated rectal administration avoided.
The use in children less than 6 months of age is not recommended, as available data in this population are limited.
IM administration: the doses used range between 0.05 and 0.15mg/kg. A total dose greater than 10 mg is usually not necessary. This route should only be used in exceptional cases. Rectal administration should be preferred as IM injection is painful.
In children less than 15kg of body weight, midazolam solutions with concentrations higher than 1mg/ml are not recommended. Higher concentrations should be diluted to 1 mg/ml.
ANAESTHESIA DOSAGE: PREMEDICATION: Premedication with midazolam given shortly before a procedure produces sedation and preoperative impairment of memory. Midazolam can also be administered in combination with anticholinergics. For this indication midazolam should be administered IV or IM, deep into a large muscle mass 20 to 60 minutes before induction of anaesthesia), or preferably via the rectal route in children. Close and continuous monitoring of the patients after administration of premedication is mandatory as interindividual sensitivity varies and symptoms of overdose may occur.
Adults: For preoperative sedation and to impair memory of preoperative events, the recommended dose for adults of ASA Physical Status I & II and below 60 years is 0.07 to 0.1mg/kg administered IM. The dose must be reduced and individualised when midazolam is administered to adults over 60 years of age, debilitated, or chronically ill patients. A dose of 0.025 to 0.05mg/kg administered IM is recommended. The usual dose is 2 to 3 mg.
Paediatric population: Neonates and children up to 6 months of age: The use in children less than 6 months of age is not recommended as available data are limited.
Children over 6 months of age: Rectal administration: The total dose of midazolam, usually ranging from 0.3 to 0.5 mg/kg should be administered 15 to 30 minutes before induction of anaesthesia. Rectal administration of the ampoule solution is performed by means of a plastic applicator fixed on the end of the syringe. If the volume to be administered is too small, water may be added up to a total volume of 10 ml.
IM administration: As IM injection is painful, this route should only be used in exceptional cases. Rectal administration should be preferred. However, a dose range from 0.08 to 0.2 mg/kg of midazolam administered IM has been shown to be effective and safe. In children between ages 1 and 15 years, proportionally higher doses are required than in adults in relation to body weight. In children less than 15 kg of body weight, midazolam solutions with concentrations higher than 1mg/ml are not recommended. Higher concentrations should be diluted to 1 mg/ml.
INDUCTION: Adults: If midazolam is used for induction of anaesthesia before other anaesthetic agents have been administered, the individual response is variable. The dose should be titrated to the desired effect according to the patient's age and clinical status. When midazolam is used before or in combination with other IV or inhalation agents for induction of anaesthesia, the initial dose of each agent should be significantly reduced, at times to as low as 25% of the usual initial dose of the individual agents. The desired level of anaesthesia is reached by stepwise titration. The IV induction dose of midazolam should be given slowly in increments. Each increment of not more than 5mg should be injected over 20 to 30 seconds allowing 2 minutes between successive increments.
In adults below the age of 60 years, an IV dose of 0.15 to 0.2 mg/kg will usually suffice. Non-premedicated adults below the age of 60 the dose usually require a higher dose (0.3 to 0.35 mg/kg IV).
If needed to complete induction, increments of approximately 25% of the patient's initial dose may be used. Induction may instead be completed with inhalational anaesthetics.
In resistant cases, a total dose of up to 0.6 mg/kg may be used for induction, but such larger doses may prolong recovery.
For Adults over 60 years of age, debilitated or chronically ill patients, the dose should be 0.1 to 0.2 mg/kg administered IV.
Non-premedicated adults over 60 years of age usually require more midazolam for induction; an initial dose of 0.15 to 0.3mg/kg is recommended. Non-premedicated patients with severe systemic disease or other debilitation usually require less midazolam for induction. An initial dose of 0.15 to 0.25mg/kg will usually suffice.
SEDATIVE COMPONENT IN COMBINED ANAESTHESIA: Adults: Midazolam can be given as a sedative component in combined anaesthesia by either further intermittent small IV doses (range between 0.03 and 0.1mg/kg) or continuous infusion of IV midazolam (range between 0.03 and 0.1 mg/kg/h) typically in combination with analgesics. The dose and the intervals between doses vary according to the patient's individual reaction.
In adults over 60 years of age, debilitated or chronically ill patients, lower maintenance doses will be required.
SEDATION IN INTENSIVE CARE UNITS (ICU): The desired level of sedation is reached by stepwise titration of midazolam followed by either continuous infusion or intermittent bolus, according to the clinical need, physical status, age and concomitant medication.
Adults: IV loading dose: 0.03 to 0.3 mg/kg should be given slowly in increments. Each increment of 1 to 2.5 mg should be injected over 20 to 30 seconds allowing 2 minutes between successive increments. In hypovolaemic, vasoconstricted, or hypothermic patients the loading dose should be reduced or omitted. When midazolam is given with potent analgesics, the latter should be administered first so that the sedative effects of midazolam can be safely titrated on top of any sedation caused by the analgesic.
IV maintenance dose: doses can range from 0.03 to 0.2 mg/kg/h. In hypovolaemic, vasoconstricted, or hypothermic patients the maintenance dose should be reduced. The level of sedation should be assessed regularly. With long-term sedation, tolerance may develop and the dose may have to be increased.
Children over 6 months of age: In intubated and ventilated paediatric patients, a loading dose of 0.05 to 0.2 mg/kg IV should be administered slowly over at least 2 to 3 minutes to establish the desired clinical effect. Midazolam should not be administered as a rapid intravenous dose. The loading dose is followed by a continuous IV infusion at 0.06 to 0.12 mg/kg/h (1 to 2 µg/kg/min). The rate of infusion can be increased or decreased (generally by 25% of the initial or subsequent infusion rate) as required or supplemental IV doses of midazolam can be administered to increase or maintain the desired effect.
When initiating an infusion with midazolam in haemodynamically compromised patients, the usual loading dose should be titrated in small increments and the patient monitored for haemodynamic instability, e.g., hypotension. These patients are also vulnerable to the respiratory depressant effects of midazolam and require careful monitoring of respiratory rate and oxygen saturation.
Neonates and children up to 6 months of age: Midazolam should be given as a continuous IV infusion, starting at 0.03 mg/kg/h (0.5 µg/kg/min) in neonates with a gestational age <32 weeks, or 0.06 mg/kg/h (1 µg/kg/min) in neonates with a gestational age >32 weeks and children up to 6 months.
Intravenous loading doses are not recommended in premature infants, neonates and children up to 6 months, rather the infusion may be run more rapidly for the first several hours to establish therapeutic plasma levels. The rate of infusion should be carefully and frequently reassessed, particularly after the first 24 hours so as to administer the lowest possible effective dose and reduce the potential for drug accumulation.
Careful monitoring of respiratory rate and oxygen saturation is required.
In premature infants, neonates and children less than 15kg of body weight, midazolam solutions with concentrations higher than 1mg/mL are not recommended. Higher concentrations should be diluted to 1 mg/mL.