


 Sign Out
Sign Out

When considering the use of TAGRISSO, EGFR mutation status should be determined using a validated test method (see Precautions) for: exon 19 deletions or exon 21 (L858R) substitution mutations (in tumour specimens for adjuvant treatment and tumour or plasma specimens for first-line treatment); T790M mutations (in tumour or plasma specimens following progression on or after EGFR TKI therapy).
Posology: The recommended dose of TAGRISSO is 80 mg osimertinib once a day.
Duration of treatment: Patients in the adjuvant setting should receive treatment until disease recurrence or unacceptable toxicity or up to a maximum of 3 years. Treatment duration for more than 3 years was not studied.
Patients with locally advanced or metastatic lung cancer should receive treatment until disease progression or unacceptable toxicity.
Missed dose: If a dose of TAGRISSO is missed, make up the dose unless the next dose is due within 12 hours.
TAGRISSO can be taken with or without food at the same time each day.
Dose adjustments: Dosing interruption and/or dose reduction may be required based on individual safety and tolerability. If dose reduction is necessary, then the dose of TAGRISSO should be reduced to 40 mg taken once daily. Dose reduction guidelines for adverse reactions toxicities are provided in Table 10. (See Table 10.)
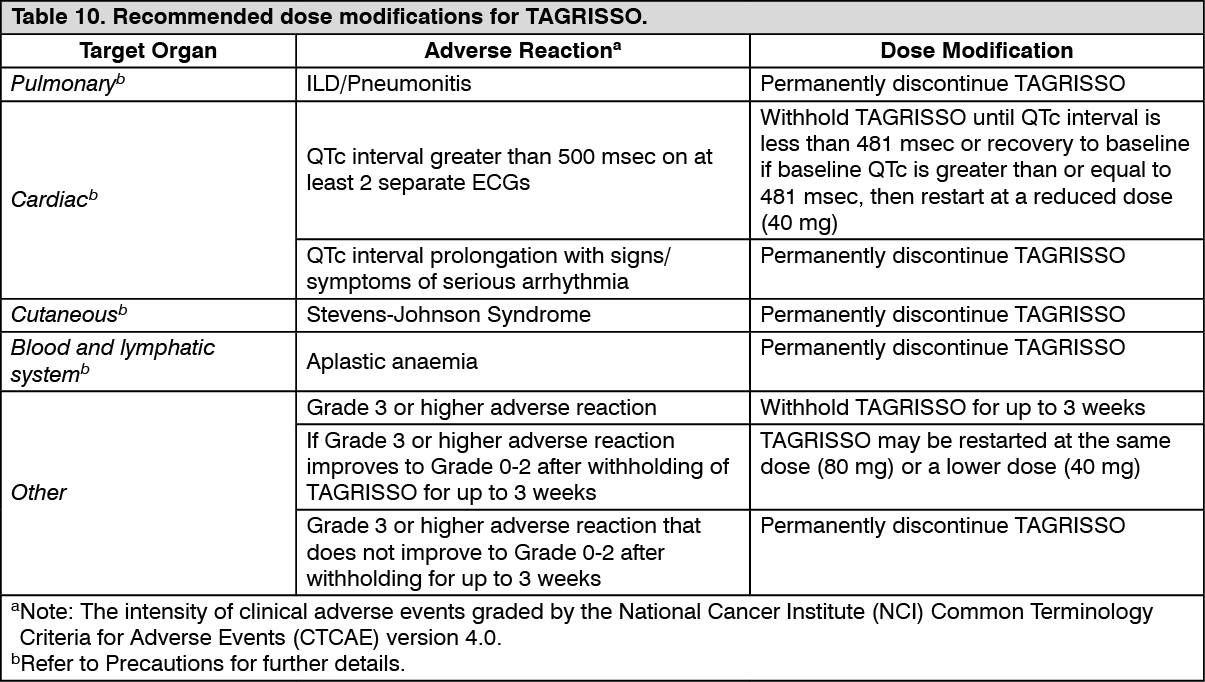 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSpecial patient populations: No dosage adjustment is required due to patient age, body weight, gender, ethnicity and smoking status (see Pharmacology: Pharmacokinetics under Actions).
Paediatric and adolescents: The safety and efficacy of TAGRISSO in children or adolescents aged less than 18 years have not been established. No data are available.
Method of administration: This medicinal product is for oral use. The tablet should be swallowed whole with water. The tablet should not be crushed, split or chewed.
If the patient is unable to swallow the tablet, it may first be dispersed in 50 mL of non-carbonated water. The tablet should be dropped in the water, without crushing, stirred until dispersed and immediately swallowed. An additional half a glass of water should be added to ensure that no residue remains and then immediately swallowed. No other liquids should be added.
If administration via nasogastric tube is required, the same process as previously mentioned should be followed but using volumes of 15 mL for the initial dispersion and 15 mL for the residue rinses. The resulting 30 mL of liquid should be administered as per the naso-gastric tube manufacturer's instructions with appropriate water flushes. The dispersion and residues should be administered within 30 minutes of the addition of the tablets to water.
Elderly (>65 years): Population pharmacokinetic (PK) analysis indicated that age did not have an impact on the exposure of osimertinib and hence, osimertinib can be used in adults without regard to age.
Hepatic impairment: Based on clinical studies, no dose adjustments are necessary in patients with mild hepatic impairment (Child Pugh A) or moderate hepatic impairment (Child Pugh B). Similarly based on population PK analysis, no dose adjustment is recommended in patients with mild hepatic impairment (total bilirubin ≤ULN and AST >ULN or total bilirubin between 1.0 to 1.5x ULN and any AST) or moderate hepatic impairment (total bilirubin between 1.5 to 3 times ULN and any AST). The appropriate dose of TAGRISSO has not been established in patients with severe hepatic impairment (see Pharmacology: Pharmacokinetics under Actions).
Renal impairment: Based on clinical studies and population PK analysis, no dose adjustments are necessary in patients with mild, moderate, or severe renal impairment. The safety and efficacy of TAGRISSO has not been established in patients with end-stage renal disease [Creatinine clearance (CLcr) less than 15 mL/min, calculated by the Cockcroft and Gault equation], or on dialysis. Caution should be exercised when treating patients with severe and end-stage renal impairment (see Pharmacology: Pharmacokinetics under Actions).