


 Sign Out
Sign Out

In vitro studies have demonstrated that TAGRISSO has high potency and inhibitory activity against EGFR across a range of all clinically relevant EGFR sensitising mutant and T790M mutant non-small cell lung cancer (NSCLC) cell lines (apparent IC50s from 6 nM to 54 nM against phospho-EGFR). This leads to inhibition of cell growth, while showing significantly less activity against EGFR in wild-type cell lines (apparent IC50s 480 nM to 1.9 μM against phospho-EGFR). In vivo oral administration of TAGRISSO lead to tumour shrinkage in both EGFRm and T790M NSCLC xenograft and transgenic mouse lung tumour models.
Based on an analysis of dose-exposure response relationships over the dose range of 20 mg (0.25 times the recommended dose) to 240 mg (3 times the recommended dose), no apparent efficacy (Objective Response Rate (ORR), Duration of Response (DoR) and Progression-Free Survival (PFS)) relationship for osimertinib was identified. Over the same dose range, increased exposure led to increased probability of adverse reactions, specifically rash, diarrhoea and ILD.
Cardiac electrophysiology: The QTc interval prolongation potential of TAGRISSO was assessed in 210 patients who received osimertinib 80 mg daily in AURA2. Serial ECGs were collected following a single dose and at steady state to evaluate the effect of TAGRISSO on QTc intervals. A pharmacokinetic/pharmacodynamic analysis with TAGRISSO predicted a drug-related QTc interval prolongation at 80 mg of 14 msec with an upper bound of 16 msec (90% CI).
Clinical efficacy and safety: Adjuvant treatment of EGFR mutation positive NSCLC, with or without prior adjuvant chemotherapy - ADAURA: The efficacy and safety of TAGRISSO for the adjuvant treatment of patients with EGFR mutation-positive (exon 19 deletions or L858R substitution mutations) NSCLC who have had complete tumour resection with or without prior adjuvant chemotherapy was demonstrated in a randomised, double-blind, placebo-controlled study (ADAURA).
Patients with resectable tumours (except for stage IA), were required to have EGFR exon 19 deletions or exon 21 L858R substitution mutations identified by the cobas EGFR Mutation Test performed prospectively using biopsy or surgical specimen in a central laboratory. The study excluded patients with clinically important ECG abnormalities identified on resting ECG (e.g. QTc interval >470 ms), history of interstitial lung disease or prior treatment with neoadjuvant or adjuvant EGFR-TKIs.
Patients were randomised (1:1) to receive TAGRISSO 80 mg orally once daily or placebo following recovery from surgery and standard adjuvant chemotherapy. Patients not receiving adjuvant chemotherapy were randomised within 10 weeks and patients receiving adjuvant chemotherapy within 26 weeks following surgery. Randomisation was stratified by mutation type (exon 19 deletions or exon 21 L858R substitution mutations), ethnicity (Asian or non-Asian) and staging based on pTNM (IB or II or IIIA) according to AJCC 7th edition. Treatment was given for 3 years or until disease recurrence or unacceptable toxicity.
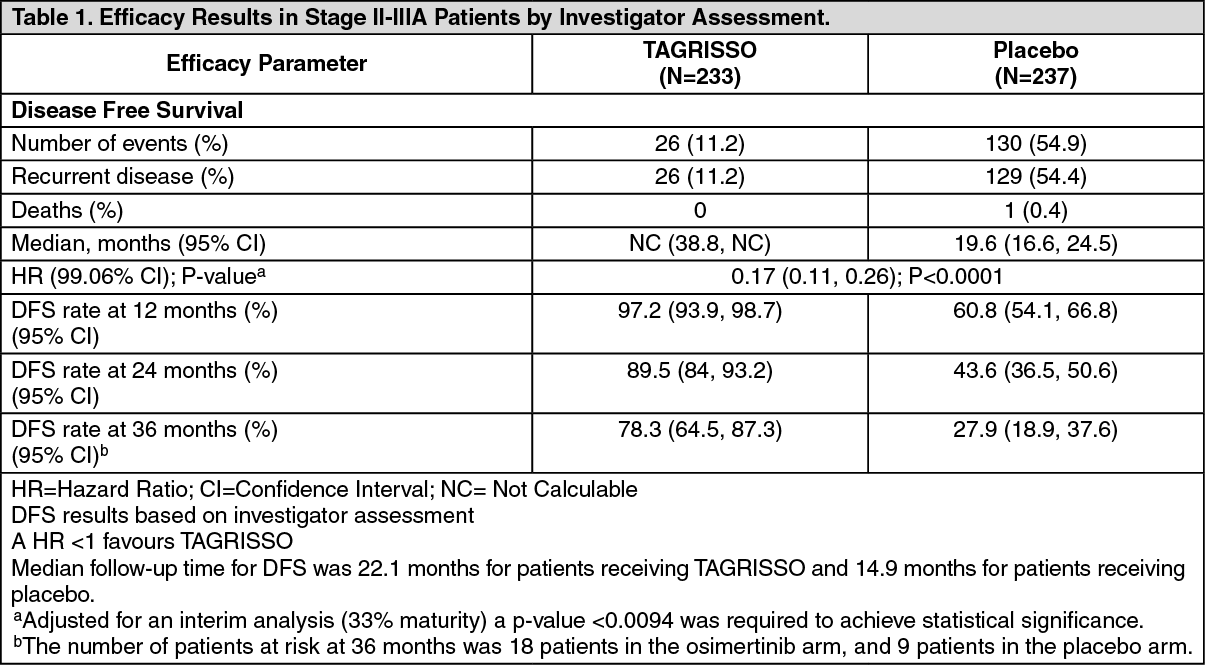
The primary efficacy outcome measure was disease-free survival (DFS) by investigator assessment for stage II-IIIA. Secondary endpoints included DFS for the overall population (stage IB-IIIA) and overall survival (OS) for stage II-IIIA and stage IB-IIIA.
A total of 682 patients were randomised to TAGRISSO (n=339) or to placebo (n=343). The median age was 63 years (range 30-86 years), 11% were ≥75 years of age; 70% were female, 64% were Asian and 72% were never smokers. Baseline WHO performance status was 0 (64%) or 1 (36%); 31% had stage IB, 34% II, and 35% IIIA. With regard to EGFR mutation status, 55% were exon 19 deletions and 45% were exon 21 L858R substitution mutations; 9 patients (1%) also had a concurrent de novo T790M mutation. The majority (60%) of patients received adjuvant chemotherapy prior to randomisation (26% IB; 71% IIA; 73% IIB; 80% IIIA).
An analysis of DFS for both the stage II-IIIA population and the overall population (IB-IIIA) was conducted. ADAURA demonstrated a statistically significant and clinically meaningful reduction in the risk of disease recurrence or death for patients treated with TAGRISSO compared to patients treated with placebo. Patients with stage II-IIIA disease treated with TAGRISSO compared to placebo, achieved 83% reduction in the risk of disease recurrence or death (median not calculated (NC) and 19.6 months, respectively, HR=0.17, 99.06% CI: 0.11, 0.26; P<0.0001). The overall population (IB-IIIA) treated with TAGRISSO compared to placebo demonstrated 80% reduction in the risk of disease recurrence or death (median NC and 27.5 months, respectively, HR=0.20, 99.12% CI: 0.14, 0.30; P<0.0001).
In the overall population, there were 37 patients who had disease recurrence on TAGRISSO. The most commonly reported sites of recurrence were: lung (19 patients); lymph nodes (10 patients) and CNS (5 patients). There were 157 patients who had disease recurrence on placebo. The most commonly reported sites were: lung (61 patients); lymph nodes (48 patients) and CNS (34 patients).
Efficacy results from ADAURA by investigator assessment are summarised in Tables 1 and 2, and the Kaplan-Meier curve for DFS in stage II-IIIA patients and in the overall population (IB-IIIA) is shown in Figure 1 and Figure 2, respectively. Overall survival (OS) data were not mature at the time of DFS analysis. (See Tables 1, 2 and Figures 1, 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image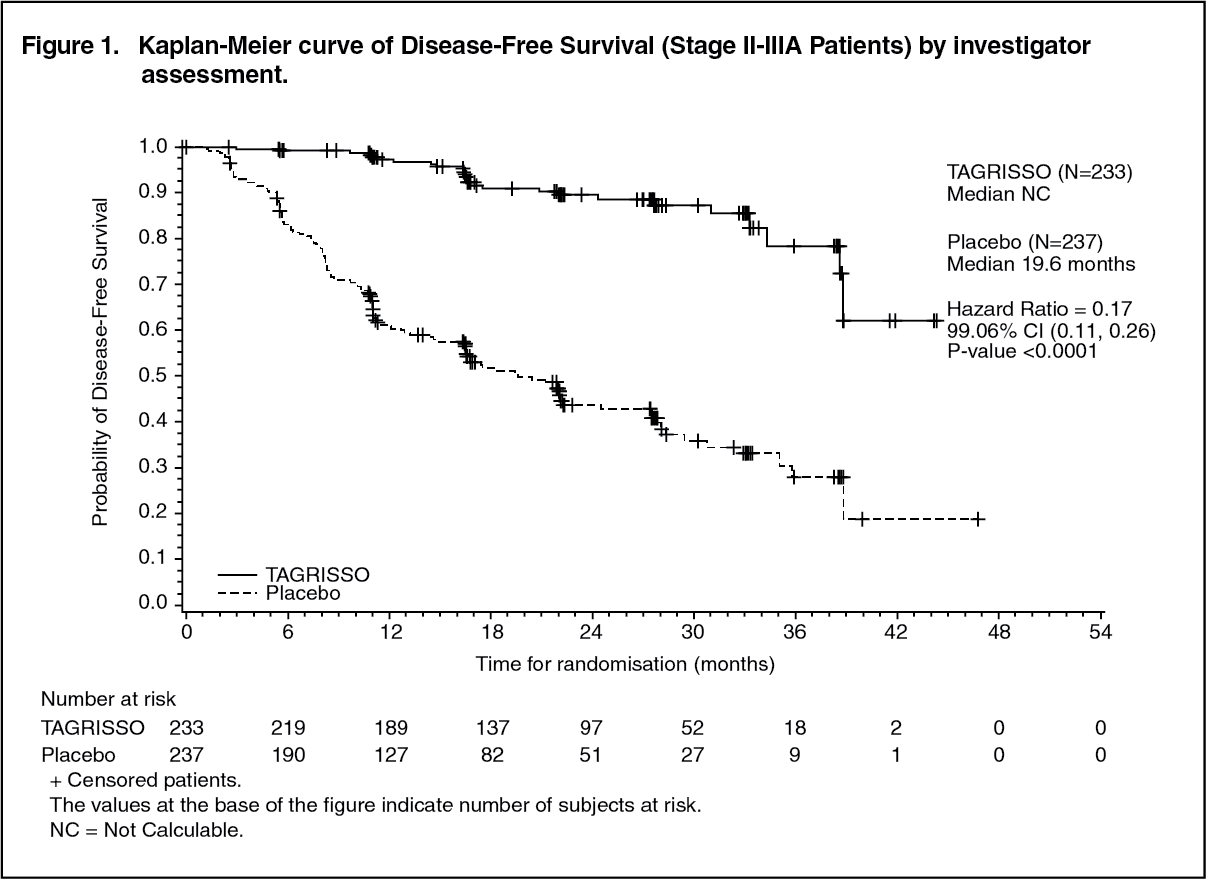 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image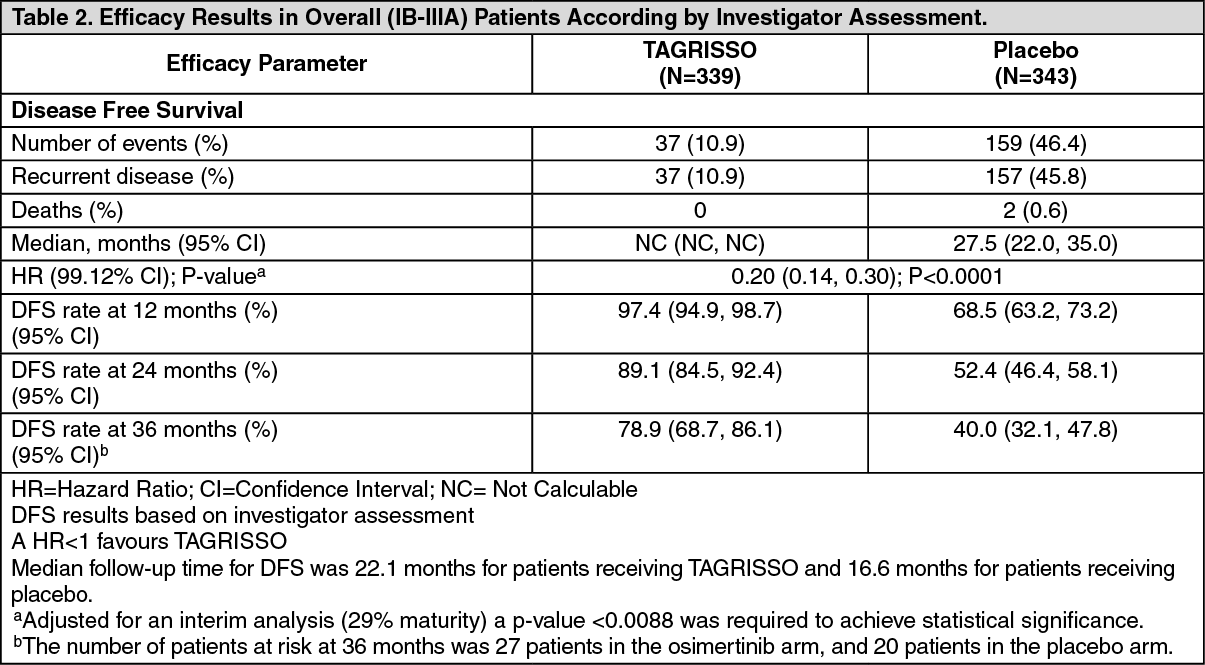 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image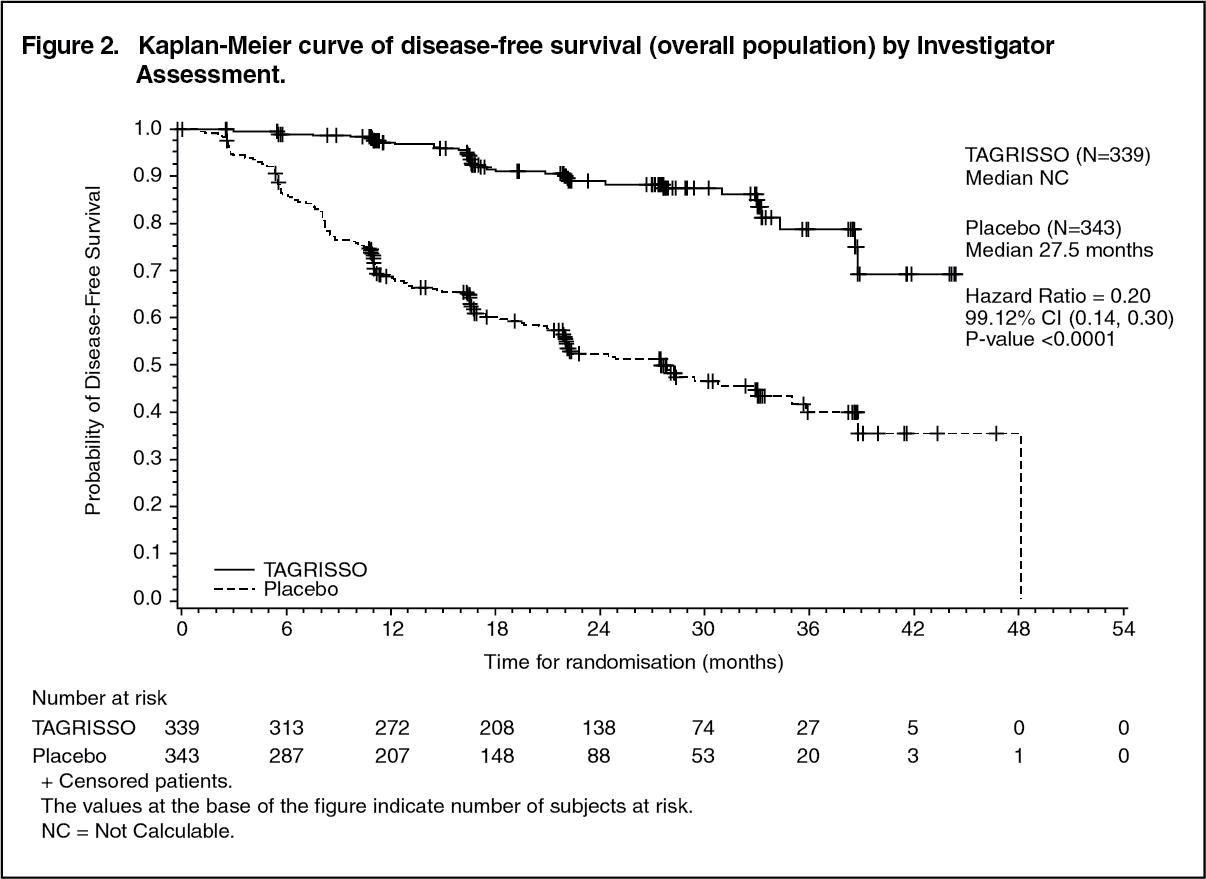 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe DFS benefit of TAGRISSO compared to placebo was consistent across all predefined subgroups analysed, including ethnicity, age, gender, and EGFR mutation type (Exon 19 deletions or L858R substitution mutations).
A clinically meaningful improvement in an exploratory analysis of CNS DFS (time to CNS recurrence or death) for patients on TAGRISSO compared to patients on placebo was observed with a HR of 0.18 (95% CI: 0.10, 0.33; P<0.0001) for the overall population, indicating a 82% reduction in the risk of CNS disease recurrence or death in the TAGRISSO arm compared to placebo.
Patient Reported Outcomes: HRQL, as measured by the Short Form (36) Health Survey version 2 (SF-36v2) questionnaire, was overall maintained in both arms, with more than 75% of stage II-IIIA patients in either arm not experiencing a clinically meaningful deterioration in the physical or mental component of the SF-36, or death. There was no difference between the arms in the time to deterioration (TTD) for the mental component of SF-36 or death (HR=0.90; 95% CI: 0.61, 1.33); median TTD of 39.0 months, 95% CI: NC, NC in the TAGRISSO arm and not reached in the placebo arm. A trend of shorter TTD for the physical component of SF-36 or death was observed in the TAGRISSO arm (HR=1.43, 95% CI: 0.96, 2.13); median TTD not reached in either arm.
Previously untreated EGFR mutation positive locally advanced or metastatic NSCLC - FLAURA: The efficacy and safety of TAGRISSO for the treatment of patients with EGFR mutation positive locally advanced or metastatic NSCLC, who had not received previous systemic treatment for advanced disease, was demonstrated in a randomised, double-blind, active-controlled study (FLAURA). Patient tumour tissue samples were required to have one of the two common EGFR mutations known to be associated with EGFR TKI sensitivity (Ex19del or L858R), as identified by local or central testing.
Patients were randomised 1:1 to receive either TAGRISSO (n=279, 80 mg orally once daily) or EGFR TKI comparator (n=277; gefitinib 250 mg orally once daily or erlotinib 150 mg orally once daily). Randomisation was stratified by EGFR mutation type (Ex19del or L858R) and ethnicity (Asian or non-Asian). Patients received study therapy until intolerance to therapy, or the investigator determined that the patient was no longer experiencing clinical benefit. For patients receiving EGFR TKI comparator, post-progression crossover to open-label TAGRISSO was permitted provided tumour samples tested positive for the T790M mutation.
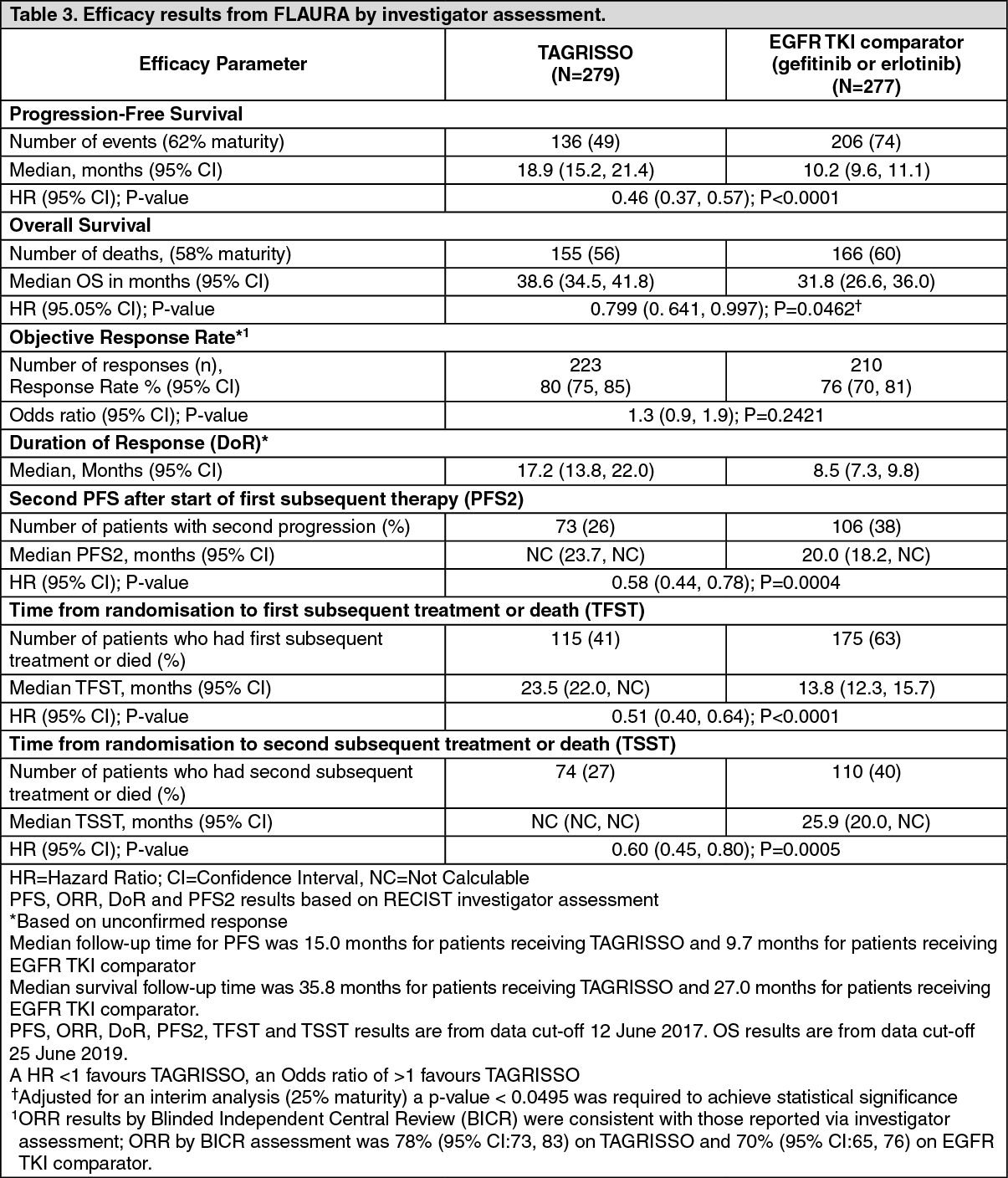
The primary efficacy end-point was progression-free survival (PFS) as assessed by investigator. Additional efficacy end-points included overall survival (OS), objective response rate (ORR), duration of response (DoR), second PFS after start of first subsequent therapy (PFS2), time to first subsequent therapy or death (TFST) and time from randomisation to second progression on subsequent treatment or death (TSST) as assessed by investigator. CNS PFS, CNS ORR and CNS DoR as assessed by BICR, and patient reported outcomes (PRO) were also assessed.
The baseline demographic and disease characteristics of the overall study population were: median age 64 years (range 26-93 years), ≥75 years old (14%), female (63%), White (36%), Asian (62%), never smokers (64%). All patients had a World Health Organization (WHO) performance status of 0 or 1. Thirty-six percent (36%) of patients had metastatic bone disease and 35% of patients had extra-thoracic visceral metastases. Twenty one percent (21%) of patients had CNS metastases (identified by CNS lesion site at baseline, medical history, and/or prior surgery, and/or prior radiotherapy to CNS metastases).
TAGRISSO demonstrated a clinically meaningful and highly statistically significant improvement in PFS compared to EGFR TKI comparator (median 18.9 months and 10.2 months, respectively, HR=0.46, 95% CI: 0.37, 0.57; P<0.0001). Efficacy results from FLAURA by investigator assessment are summarised in Table 3, and the Kaplan-Meier curve for PFS is shown in Figure 3. The final analysis of overall survival (58% maturity) demonstrated a statistically significant improvement with an HR of 0.799 (95.05% CI: 0.641, 0.997; P = 0.0462) and a clinically meaningful longer median survival time in patients randomised to TAGRISSO compared to EGFR TKI comparator (Table 3 and Figure 4). A greater proportion of patients treated with TAGRISSO were alive at 12, 18, 24 and 36 months (89%, 81%, 74% and 54%, respectively) compared to patients treated with EGFR TKI comparator (83%, 71%, 59% and 44%, respectively). (See Table 3 and Figures 3, 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image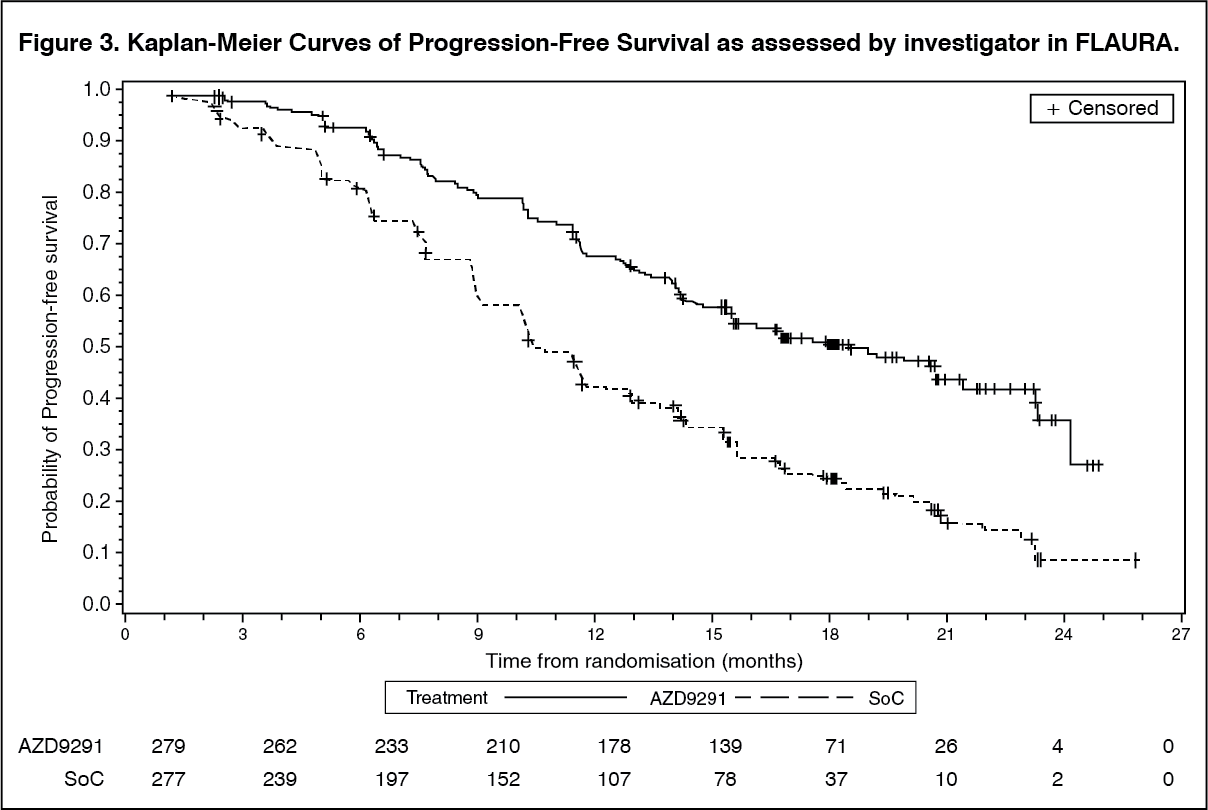 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image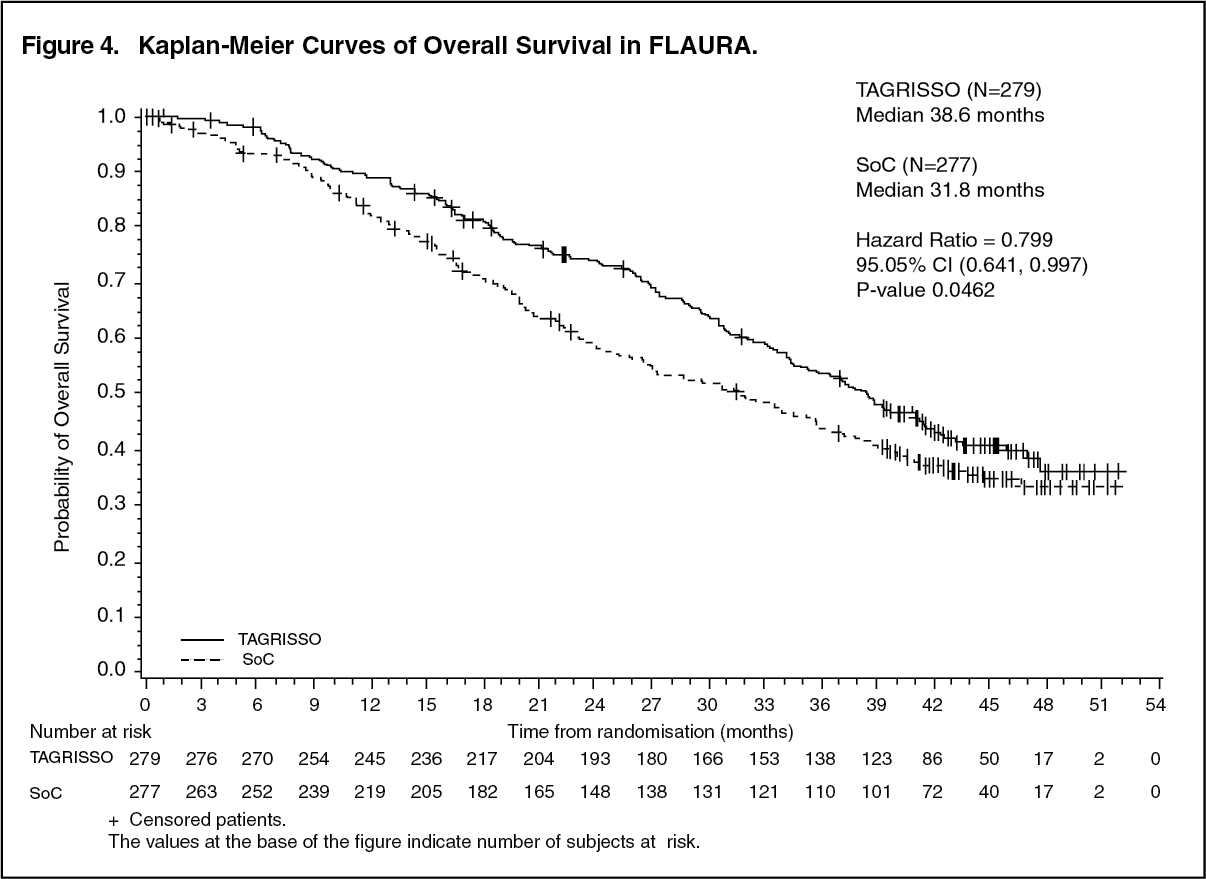 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe PFS benefit of TAGRISSO compared to EGFR TKI comparator was consistent across all predefined subgroups analysed, including ethnicity, age, gender, smoking history, CNS metastases status at study entry and EGFR mutation type (Exon 19 deletion or L858R).
Patients randomised to TAGRISSO as first-line treatment also had clinically meaningful improvements in PFS2, TFST and TSST compared to patients randomised to EGFR TKI comparator. The analysis of these post-progression end-points demonstrated that PFS benefit was largely preserved through subsequent lines of therapy.
In patients with locally advanced EGFRm NSCLC not amenable to curative surgery or radiotherapy, the objective response rate was 93% (95% CI 66, 100) for patients receiving TAGRISSO (n=14) and 60% (95% CI 32, 84) for patients receiving EGFR TKI comparator (n=15).
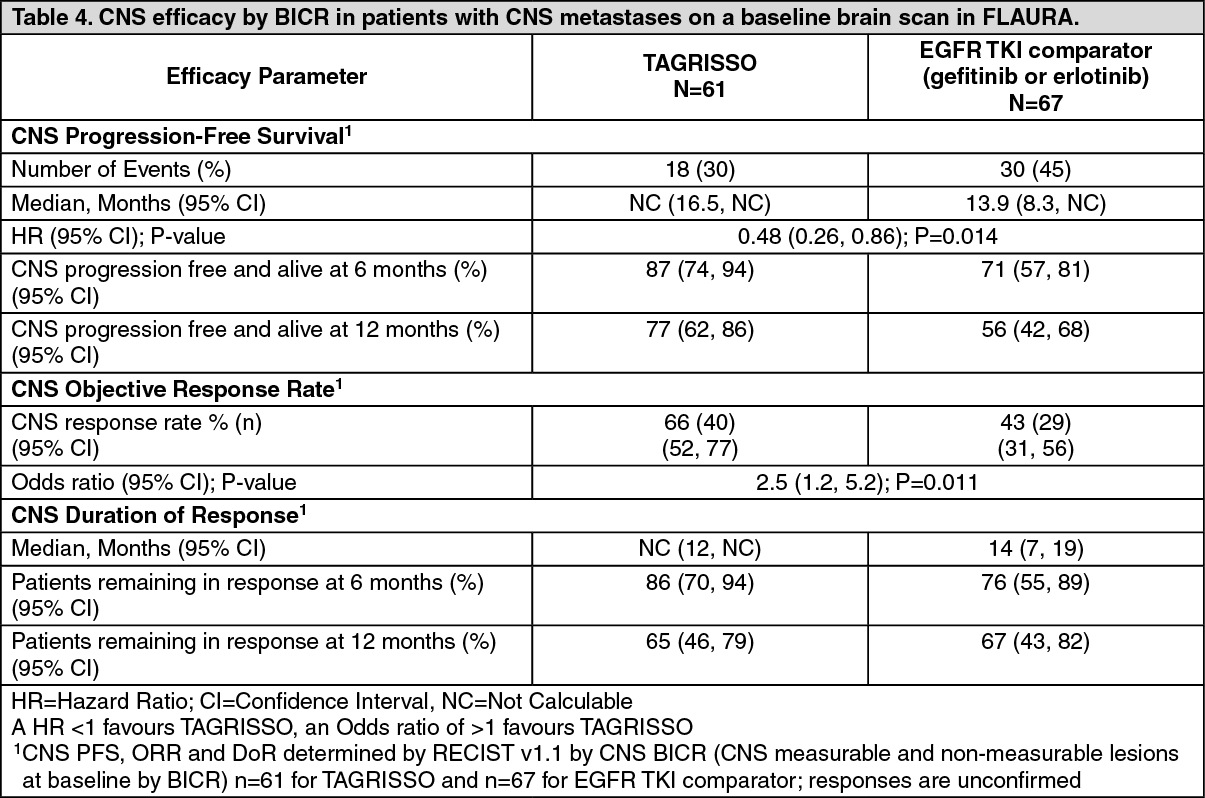
CNS metastases efficacy data in FLAURA study: Patients with CNS metastases not requiring steroids and with stable neurologic status for at least two weeks after completion of the definitive therapy and steroids were eligible to be randomised in the FLAURA study. Of 556 patients, 200 patients had available baseline brain scans. A BICR assessment of these scans resulted in a subgroup of 128/556 (23%) patients with CNS metastases and these data are summarised in Table 4. EGFR mutation type (Ex19del or L858R) and ethnicity (Asian or non-Asian) was generally balanced within this analysis between the treatment arms. CNS efficacy by RECIST v1.1 in FLAURA demonstrated a statistically significant improvement in CNS PFS (HR=0.48, 95% CI 0.26, 0.86; P=0.014). (See Table 4.)
 Click on icon to see table/diagram/image
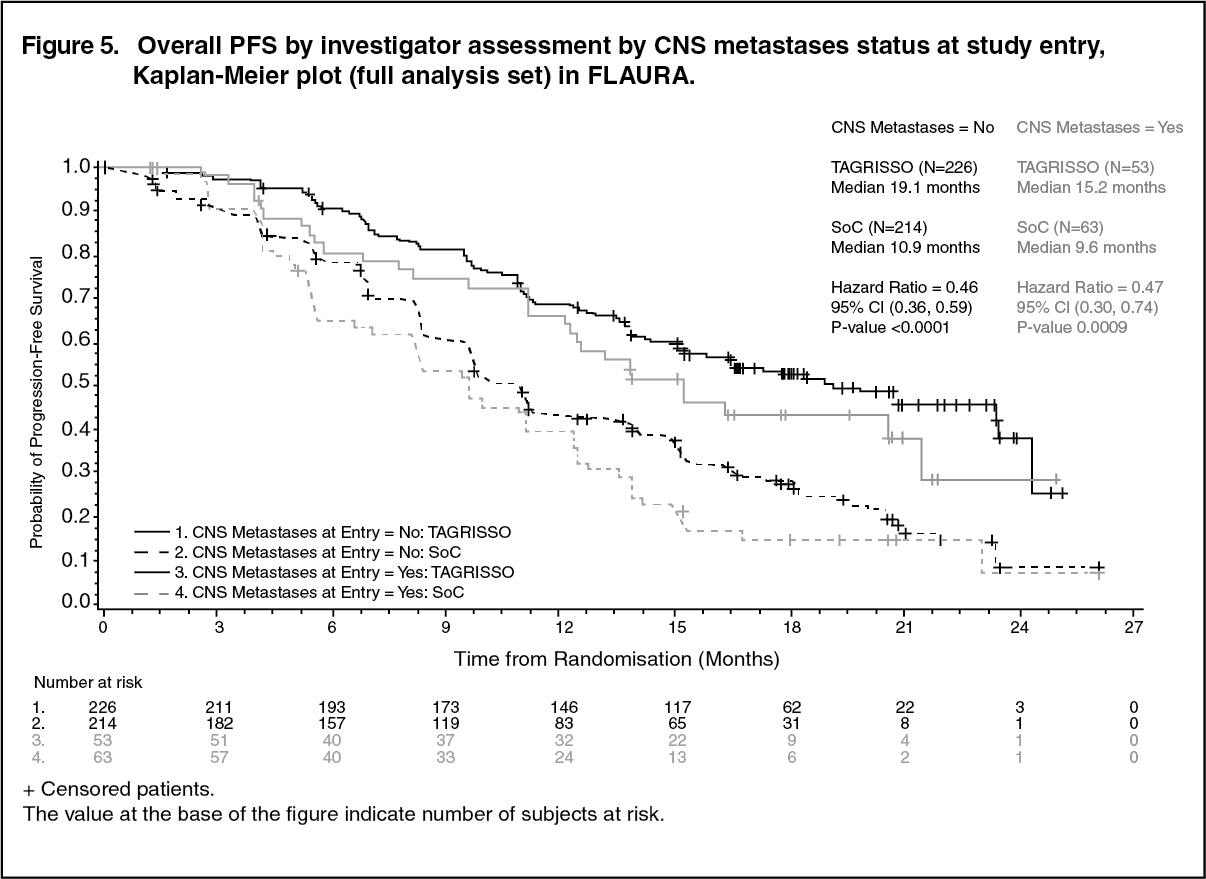
Click on icon to see table/diagram/imageA pre-specified PFS subgroup based on CNS metastases status (identified by CNS lesion site at baseline, medical history, and/or prior surgery, and/or prior radiotherapy to CNS metastases) at study entry was performed in FLAURA and is shown in Figure 5. Irrespective of CNS lesion status at study entry, patients in the TAGRISSO arm demonstrated an efficacy benefit over those in the EGFR TKI comparator arm. (See Figure 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIrrespective of CNS lesion status at study entry, based on investigator assessment, there were fewer patients with new CNS lesions in the TAGRISSO arm compared to the EGFR TKI comparator arm (TAGRISSO, 11/279 [3.9%] compared to EGFR TKI comparator, 34/277 [12.3%]). In the subset of patients without CNS lesions at baseline, there were a lower number of new CNS lesions in the TAGRISSO arm compared to the EGFR TKI comparator arm (7/226 [3.1%] vs. 15/214 [7.0%], respectively).
Patient Reported Outcomes (PRO): Patient-reported symptoms and health-related quality of life (HRQL) were electronically collected using the EORTC QLQ-C30 and its lung cancer module (EORTC QLQ-LC13). The LC13 was initially administered once a week for the first 6 weeks, then every 3 weeks before and after progression. The C30 was assessed every 6 weeks before and after progression. At baseline, no differences in patient reported symptoms, function or HRQL were observed between TAGRISSO and EGFR TKI comparator (gefitinib or erlotinib) arms. Compliance over the first 9 months was generally high (≥70%) and similar in both arms.
Key lung cancer symptoms analysis: Data collected from baseline up to month 9 showed similar improvements in TAGRISSO and EGFR TKI comparator groups for the five pre-specified primary PRO symptoms (cough, dyspnoea, chest pain, fatigue, and appetite loss) with improvement in cough reaching the established clinically relevant cutoff. Up to month 9 there were no clinically meaningful differences in patient-reported symptoms between TAGRISSO and EGFR TKI comparator groups (as assessed by a difference of ≥ 10 points). Data are presented in Table 5. (See Table 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageHRQL and physical functioning improvement analysis: Both groups reported similar improvements in most functioning domains and global health status/HRQL, indicating that patients overall health status improved. Up to month 9, there were no clinically meaningful differences between the TAGRISSO and EGFR TKI comparator groups in functioning or HRQL.
Pretreated T790M positive NSCLC patients - AURA3: The efficacy and safety of TAGRISSO for the treatment of patients with locally advanced or metastatic T790M NSCLC whose disease has progressed on or after EGFR TKI therapy, was demonstrated in a randomised, open label, active-controlled Phase 3 study (AURA3). All patients were required to have EGFR T790M mutation positive NSCLC identified by the cobas EGFR mutation test performed in a central laboratory prior to randomisation. The T790M mutation status was also assessed using ctDNA extracted from a plasma sample taken during screening. The primary efficacy outcome was progression-free survival (PFS) as assessed by investigator. Additional efficacy outcome measures included Objective Response Rate (ORR), Duration of Response (DoR), Disease Control Rate (DCR) and Overall Survival (OS) as assessed by investigator.
Patients were randomised in a 2:1 (TAGRISSO: platinum-based doublet chemotherapy) ratio to receive TAGRISSO (n=279) or platinum-based doublet chemotherapy (n=140). Randomisation was stratified by ethnicity (Asian and non-Asian). Patients in the TAGRISSO arm received TAGRISSO 80 mg orally once daily until intolerance to therapy, or the investigator determined that the patient was no longer experiencing clinical benefit. Chemotherapy consisted of pemetrexed 500 mg/m2 with carboplatin AUC5 or pemetrexed 500 mg/m2 with cisplatin 75 mg/m2 on day 1 of every 21 day cycle for up to 6 cycles. Patients whose disease had not progressed after four cycles of platinum-based chemotherapy could receive pemetrexed maintenance therapy (pemetrexed 500 mg/m2 on day 1 of every 21 day cycle). Subjects on the chemotherapy arm who had objective radiological progression (by the investigator and confirmed by independent central imaging review) were given the opportunity to begin treatment with TAGRISSO.
The baseline demographic and disease characteristics of the overall study population were: median age 62 years, 15% of patients were ≥ 75 years old, female (64%), white (32%), Asian (65%). Sixty-eight percent (68%) of patients were never smokers, 100% of patients had a World Health Organization (WHO) performance status of 0 or 1. Fifty-four percent (54%) of patients had extra-thoracic visceral metastases, including 34% with CNS metastases (identified by CNS lesion site at baseline, medical history, and/or prior surgery, and/or prior radiotherapy to CNS metastases) and 23% with liver metastases. Forty-two percent (42%) of patients had metastatic bone disease.
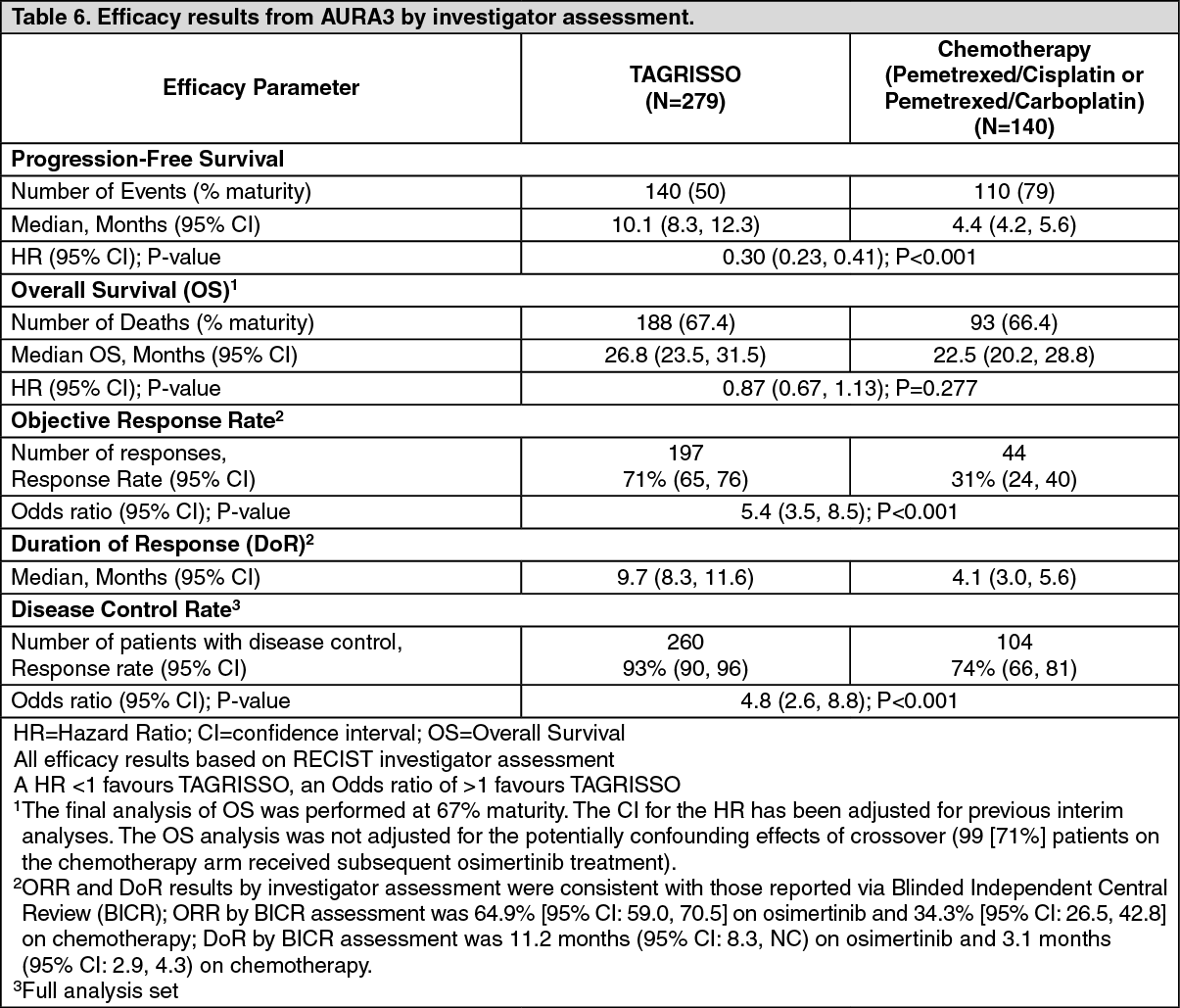
AURA3 demonstrated a statistically significant improvement in PFS in the patients treated with TAGRISSO compared to chemotherapy. Efficacy results from AURA3 by investigator assessment are summarised in Table 6, and the Kaplan-Meier curve for PFS is shown in Figure 6. No statistically significant difference was observed between the treatment arms at the final OS analysis (conducted at 67% maturity), at which time 99 patients (71%) randomised to chemotherapy had crossed over to TAGRISSO treatment. (See Table 6 and Figure 6.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image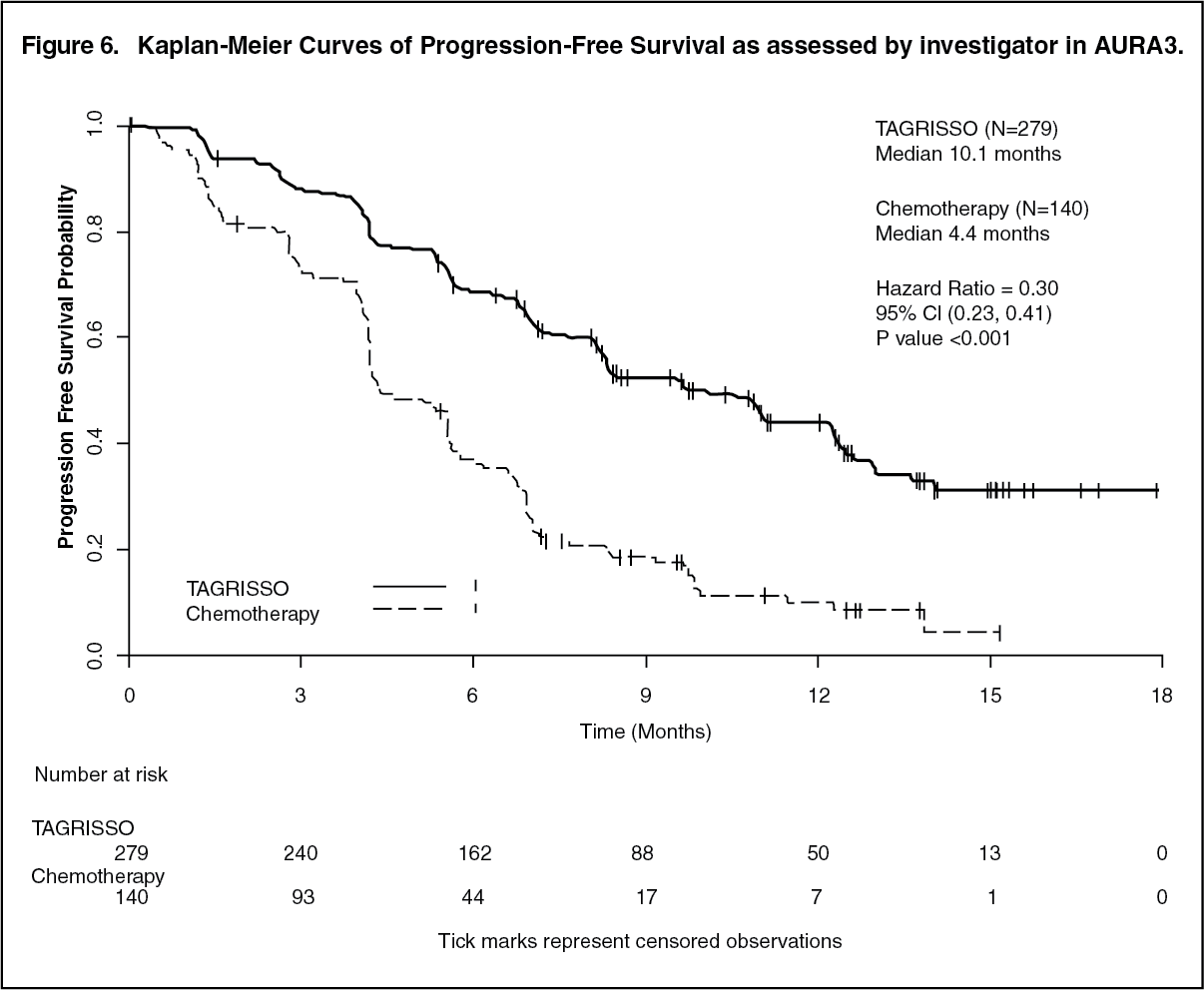 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageA sensitivity analysis of PFS was conducted by a Blinded Independent Central Review (BICR) and showed a median PFS of 11.0 months with TAGRISSO compared with 4.2 months with chemotherapy. This analysis demonstrated a consistent treatment effect (HR 0.28; 95% CI: 0.20, 0.38) with that observed by investigator assessment.
Clinically meaningful improvements in PFS with HRs less than 0.50 in favour of patients receiving TAGRISSO compared to those receiving chemotherapy were consistently observed in all predefined subgroups analysed, including ethnicity, age, gender, smoking history, CNS metastases status at study entry, EGFR mutation (Exon 19 deletion and L858R), and duration of first-line therapy with an EGFR TKI.
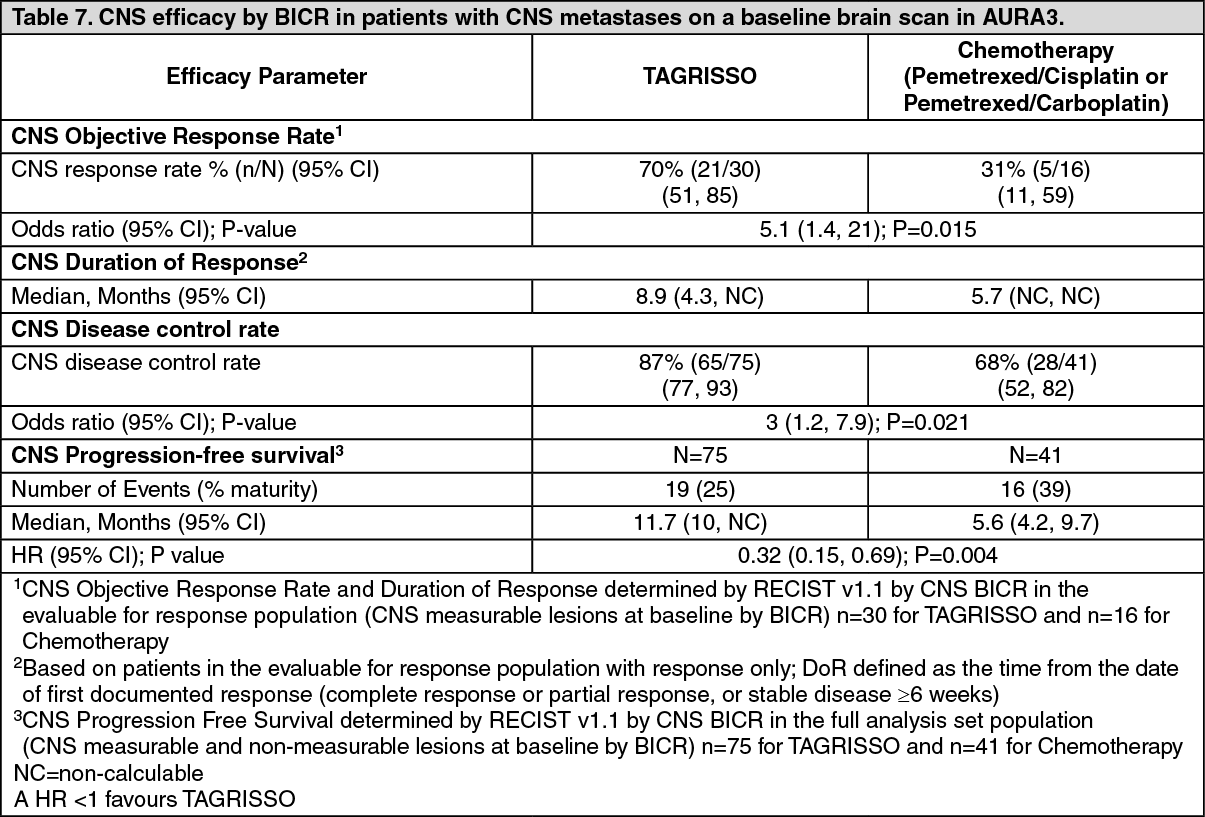
CNS metastases efficacy data in AURA3 study: Patients with asymptomatic, stable brain metastases not requiring steroids for at least 4 weeks prior to the start of study treatment were eligible to be randomised in the study. A BICR assessment of CNS efficacy by RECIST v1.1 in the subgroup of 116/419 (28%) patients identified to have CNS metastases on a baseline brain scan are summarised in Table 7. CNS responses were observed irrespective of prior brain radiation status. (See Table 7.)
 Click on icon to see table/diagram/image
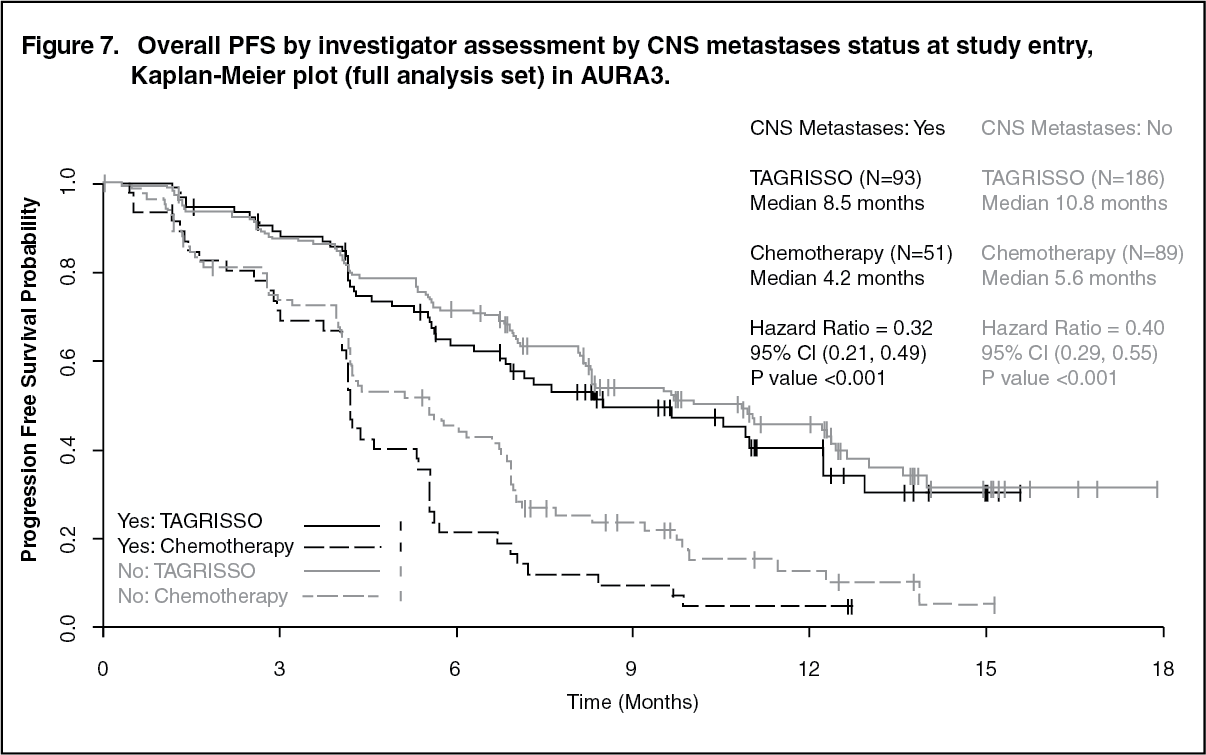
Click on icon to see table/diagram/imageA pre-specified PFS subgroup analysis based on CNS metastases status at study entry was performed in AURA3 and is shown in Figure 7 and Table 8. (See Figure 7 and Table 8.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image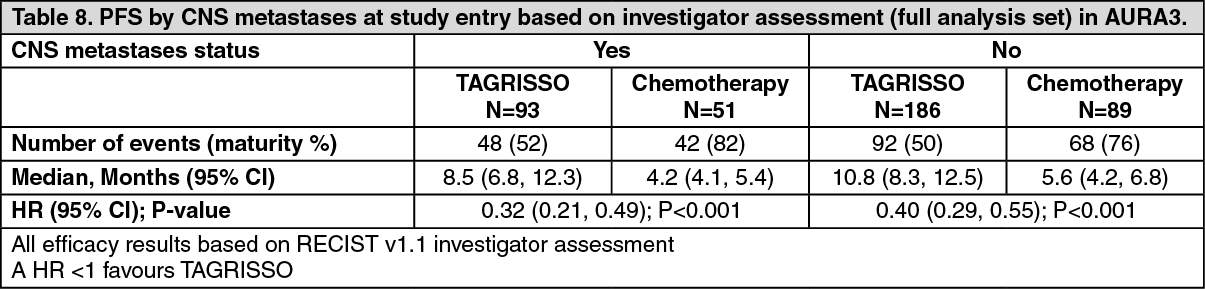 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAURA3 demonstrated an improvement in PFS for patients receiving TAGRISSO compared to those receiving chemotherapy irrespective of CNS metastases status at study entry.
TAGRISSO decreased the appearance of new CNS metastases (4.7%) as compared with chemotherapy (14.3%) according to RECIST v1.1 by investigator assessment.
Patient Reported Outcomes: Patient-reported symptoms and health-related quality of life (HRQL) were electronically collected using the EORTC QLQ-C30 and its lung cancer module (EORTC QLQ-LC13). The LC13 was initially administered once a week for the first 6 weeks, then every 3 weeks before and after progression. The C30 was assessed every 6 weeks before and after progression.
Key lung cancer symptoms analysis: TAGRISSO improved patient-reported lung cancer symptoms compared to chemotherapy by demonstrating a statistically significant difference in mean change from baseline versus chemotherapy during the overall time period from randomisation until 6 months for 5 pre-specified primary PRO symptoms (appetite loss, cough, chest pain, dyspnoea, and fatigue) as shown in Table 9. (See Table 9.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageHRQL and physical functioning improvement analysis: Patients on TAGRISSO had significantly greater chances of achieving a clinically meaningful improvement of greater than or equal to 10 points on the global health status and physical functioning of the EORTC-C30 questionnaire compared with chemotherapy during the study period Odds Ratio (OR) global health status: 2.11, (95% CI 1.24, 3.67, p=0.007); OR physical functioning 2.79 (95% CI 1.50, 5.46, p=0.002).
Pretreated T790M positive NSCLC patients - AURAex and AURA2: Two single-arm, open-label clinical studies, AURAex (Phase 2 Extension cohort, (n=201)) and AURA2 (n=210) were conducted in patients with EGFR T790M mutation positive lung cancer who have progressed on one or more prior systemic therapies, including an EGFR TKI. All patients were required to have EGFR T790M mutation positive NSCLC identified by an EGFR mutation test performed in a central laboratory prior to dosing. T790M mutation status was also assessed retrospectively using ctDNA extracted from a plasma sample taken during screening. All patients received TAGRISSO at a dose of 80 mg once daily. The primary efficacy outcome measure of these two trials was objective response rate (ORR) according to RECIST v1.1 as evaluated by a Blinded Independent Central Review (BICR). Secondary efficacy outcome measures included Duration of Response (DoR) and Progression-Free Survival (PFS).
Baseline characteristics of the overall study population (AURAex and AURA2) were as follows: median age 63 years, 13% of patients were ≥75 years old, female (68%), White (36%), Asian (60%). Majority of the subjects (96.7%) recruited were of the adenocarcinoma subtype. All patients received at least one prior line of therapy. 31% (N=129) had received 1 prior line of therapy (EGFR-TKI treatment only, second-line, chemotherapy naïve), 69% (N=282) had received 2 or more prior lines. Seventy-two percent (72%) of patients were never smokers, 100% of patients had a World Health Organization (WHO) performance status of 0 or 1. Fifty-nine percent (59%) of patients had extra-thoracic visceral metastasis including 39% with CNS metastases (identified by CNS lesion site at baseline, medical history, and/or prior surgery and/or prior radiotherapy to CNS metastases) and 29% with liver metastases. Forty-seven percent (47%) of patients had metastatic bone disease. The median duration of follow up for PFS was 12.6 months.
In the 411 pre-treated EGFR T790M mutation positive patients, the ORR by BICR in the evaluable for response population was 66% (95% CI: 61, 71). In patients with a confirmed response by BICR, the median DoR was 12.5 months (95% CI: 11.1, NE). The median PFS by BICR was 11.0 months 95% CI (9.6, 12.4).
Objective response rates by BICR above 50% were observed in all predefined subgroups analysed, including line of therapy, race, age and region. The ORR by BICR in AURAex was 62% (95% CI: 55, 68) and 70% (95% CI: 63, 77) in AURA2.
Among the patients in the evaluable for response population with objective responses, 85% (223/262) had documentation of response at the time of the first scan (6 weeks); 94% (247/262) had documentation of response at the time of the second scan (12 weeks).
CNS metastases efficacy data in Phase 2 studies (AURAex and AURA2): A BICR assessment of CNS efficacy by RECIST v1.1 was performed in a subgroup of 50 (out of 411) patients identified to have measurable CNS metastases on a baseline brain scan. A CNS ORR of 54% (27/50 patients; 95% CI: 39.3, 68.2) was observed with 12% being complete responses.
Pharmacokinetics: Osimertinib pharmacokinetic parameters have been characterised in healthy subjects and NSCLC patients. Based on population pharmacokinetic analysis, osimertinib apparent plasma clearance is 14.3 L/h, apparent volume of distribution is 918 L and terminal half-life of approximately 44 hours. The AUC and Cmax increased dose proportionally over 20 to 240 mg dose range. Administration of TAGRISSO once daily results in approximately 3-fold accumulation with steady-state exposures achieved by 15 days of dosing. At steady state, circulating plasma concentrations are typically maintained within a 1.6 fold range over the 24-hour dosing interval.
Absorption: Following oral administration of TAGRISSO, peak plasma concentrations of osimertinib was achieved with a median (min-max) tmax of 6 (3-24) hours, with several peaks observed over the first 24 hours in some patients. The absolute bioavailability of TAGRISSO is 70% (90% CI 67, 73). Based on a clinical pharmacokinetic study in patients at 80 mg, food does not alter osimertinib bioavailability to a clinically meaningful extent. (AUC increase 6% (90% CI -5, 19) and Cmax decrease -7% (90% CI -19, 6)). In healthy volunteers administered an 80 mg tablet where gastric pH was elevated by dosing of omeprazole for 5 days, osimertinib exposure was not affected (AUC and Cmax increase by 7% and 2%, respectively) with the 90% CI for exposure ratio contained within the 80-125% limit.
Distribution: Population estimated mean volume of distribution at steady state (Vss/F) of osimertinib is 918 L indicating extensive distribution into tissue. In vitro, plasma protein binding of osimertinib is 94.7% (5.3% free). Osimertinib has also been demonstrated to bind covalently to rat and human plasma proteins, human serum albumin and rat and human hepatocytes.
Biotransformation: In vitro studies indicate that osimertinib is metabolised predominantly by CYP3A4, and CYP3A5. Based on in vitro studies, 2 pharmacologically active metabolites (AZ7550 and AZ5104) have subsequently been identified in the plasma of preclinical species and in humans after oral dosing with TAGRISSO; AZ7550 showed a similar pharmacological profile to TAGRISSO while AZ5104 showed greater potency across both mutant and wild-type EGFR. Both metabolites appeared slowly in plasma after administration of TAGRISSO to patients, with a median (min-max) tmax of 24 (4-72) and 24 (6-72) hours, respectively. In human plasma, parent osimertinib accounted for 0.8%, with the 2 metabolites contributing 0.08% and 0.07% of the total radioactivity with the majority of the radioactivity being covalently bound to plasma proteins. The geometric mean exposure of both AZ5104 and AZ7550, based on AUC, was approximately 10% each of the exposure of osimertinib at steady state.
The main metabolic pathway of osimertinib was oxidation and dealkylation. At least 12 components were observed in the pooled urine and faecal samples in humans with 5 components accounting for >1% of the dose of which unchanged osimertinib, AZ5104 and AZ7550, accounted for approximately 1.9, 6.6 and 2.7% of the dose while a cysteinyl adduct (M21), and an unknown metabolite (M25) accounted for 1.5% and 1.9% of the dose, respectively.
Based on in vitro studies, osimertinib is a competitive inhibitor of CYP 3A4/5 but not CYP 1A2, 2A6, 2B6, 2C8, 2C9, 2C19, 2D6 and 2E1 at clinically relevant concentrations. Based on in vitro studies, osimertinib is not an inhibitor of UGT1A1 and UGT2B7 at clinically relevant concentrations hepatically. Intestinal inhibition of UGT1A1 is possible but the clinical impact is unknown.
Elimination: Following a single oral dose of 20 mg, 67.8% of the dose was recovered in faeces (1.2% as parent) while 14.2% of the administered dose (0.8% as parent) was found in urine by 84 days of sample collection. Unchanged osimertinib accounted for approximately 2% of the elimination with 0.8% in urine and 1.2% in faeces.
Interactions with transport proteins: In vitro studies have shown that osimertinib is not a substrate of OATP1B1 and OATP1B3.
In vitro, osimertinib does not inhibit P-gp, OAT1, OAT3, OATP1B1, OATP1B3, MATE1, MATE2K and OCT2 at clinically relevant concentrations.
Effects of osimertinib on P-gp and BCRP: Based on in vitro studies, osimertinib is a substrate of P-gp BCRP, but is unlikely to result in clinically relevant drug interactions with active substances by osimertinib at the clinical doses. Based on in vitro data, osimertinib is an inhibitor of BCRP (see Interactions).
Special populations: In a population based PK analysis (n=1367), no clinically significant relationships were identified between predicted steady-state exposure (AUCss) and patient's age (range: 25 to 91 years), gender (65% female), ethnicity (including white, Asian, Japanese, Chinese and non-Asian-non-white patients), line of therapy and smoking status (n=34 current smokers, n=419 former smokers). Population PK analysis indicated that body weight was a significant covariate with a less than 20% change in osimertinib AUCss expected across a body weight range of 88 kg to 43 kg respectively (95% to 5% quantiles) when compared to the AUCss for the median body weight of 61 kg. Taking the extremes of body weight into consideration, from <43 kg to >88 kg, AZ5104 metabolite ratios ranged from 11.8% to 9.6% while for AZ7550 it ranged from 12.8% to 8.1%, respectively. Based on population PK analysis, serum albumin was identified as a significant covariate with a <30% change in osimertinib AUCss expected across the albumin range of 29 to 46 g/L respectively (95% to 5% quantiles) when compared to the AUCss for the median baseline albumin of 39 g/L. These exposure changes due to body weight or baseline albumin differences are not considered clinically relevant.
Hepatic impairment: Osimertinib is eliminated mainly via the liver. In a clinical trial, patients with mild hepatic impairment (Child Pugh A, n=7) or moderate hepatic impairment (Child Pugh B, n=5) had no increase in exposure compared to patients with normal hepatic function (n=10) after a single 80 mg dose of TAGRISSO. Based on population PK analysis, there was no relationship between markers of hepatic function (ALT, AST, bilirubin) and osimertinib exposure. The hepatic impairment marker serum albumin showed an effect on the PK of osimertinib. Clinical studies that were conducted excluded patients with AST or ALT >2.5x upper limit of normal (ULN), or if due to underlying malignancy, >5.0x ULN or with total bilirubin >1.5x ULN. Based on a pharmacokinetic analysis of 134 patients with mild hepatic impairment (total bilirubin ≤ULN and AST >ULN or total bilirubin between 1.0 to 1.5x ULN and any AST), 8 patients with moderate hepatic impairment (total bilirubin between 1.5 times to 3.0 times ULN and any AST) and 1216 patients with normal hepatic function (total bilirubin less than or equal to ULN and AST less than or equal to ULN), osimertinib exposures were similar. There are no data available on patients with severe hepatic impairment (see Dosage & Administration).
Renal impairment: In a clinical trial, patients with severe renal impairment (CLcr 15 to less than 30 mL/min; n=7) compared to patients with normal renal function (CLcr greater than or equal to 90 mL/min; n=8) after a single 80 mg dose of TAGRISSO showed a 1.85-fold increase in AUC (90% CI: 0.94, 3.64) and a 1.19-fold increase in Cmax (90% CI: 0.69, 2.07). Furthermore, based on a population PK analysis of 593 patients with mild renal impairment (CLcr 60 to less than 90 mL/min), 254 patients with moderate renal impairment (CLcr 30 to less than 60 mL/min), 5 patients with severe renal impairment (CLcr 15 to less than 30 mL/min) and 502 patients with normal renal function (greater than or equal to 90 mL/min), osimertinib exposures were similar. Patients with CLcr less than or equal to 10 mL/min were not included in the clinical trials.
Patients with brain metastases: In a microdose PET study in EGFR mutation positive NSCLC patients (n=4) with brain metastases, brain penetration and distribution of osimertinib was achieved at a median Tmax of 22 min and a mean Cmax of 1.5% injected dose reached the brain. This was similar to that observed in a healthy volunteers study (n=7; Tmax: 11 min; Cmax: 2.2% of injected dose reached the brain).
Toxicology: Preclinical safety data: Repeat dose toxicity: The main findings observed in repeat dose toxicity studies in rats and dogs comprised atrophic, inflammatory and/or degenerative changes affecting the epithelia of the eye (cornea), GI tract (including tongue), skin, and male and female reproductive tracts. These findings occurred at plasma concentrations that were below those seen in patients at the 80 mg therapeutic dose. The findings present following 1 month of dosing were largely reversible within 1 month of cessation of dosing.
Lens fibre degeneration was observed in the 104-week carcinogenicity rat study at exposures 0.2-times the AUC observed at the recommended clinical dose of 80 mg once daily and was consistent with the ophthalmoscopic observation of lens opacities which were first noted from week 52 and showed a gradual increase in incidence and severity with increased duration of dosing.
Carcinogenesis and mutagenesis: Osimertinib showed no carcinogenic potential when administered orally to Tg rasH2 transgenic mice for 26 weeks. An increased incidence of proliferative vascular lesions (angiomatous hyperplasia and haemangioma) in the mesenteric lymph node was observed in the rat 104-week carcinogenicity study at exposures 0.2-times the AUC observed at the recommended clinical dose of 80 mg once daily. Osimertinib did not cause genetic damage in in vitro and in vivo assays.
Reproductive toxicology: Based on studies in animals, male fertility may be impaired by treatment with TAGRISSO. Degenerative changes were present in the testes in rats and dogs exposed to osimertinib for ≥1 month and there was a reduction in male fertility in rats following exposure to osimertinib for 3 months. These findings were seen at clinically relevant plasma concentrations. Pathology findings in the testes seen following 1 month dosing were reversible in rats, however, a definitive statement on reversibility of these lesions in dogs cannot be made.
Based on studies in animals, female fertility may be impaired by treatment with TAGRISSO. In repeat dose toxicity studies, an increased incidence of anoestrus, corpora lutea degeneration in the ovaries and epithelial thinning in the uterus and vagina were seen in rats exposed to osimertinib for ≥1 month at clinically relevant plasma concentrations. Findings in the ovaries seen following 1 month dosing were reversible. In a female fertility study in rats, administration of osimertinib at 20 mg/kg/day (approximately equal to the recommended daily clinical dose of 80 mg) had no effects on oestrus cycling or the number of females becoming pregnant, but caused early embryonic deaths. These findings showed evidence of reversibility following a 1 month off-dose.
In a modified embryofoetal development study in the rat, osimertinib caused embryolethality when administered to pregnant rats prior to embryonic implantation. These effects were seen at a maternally tolerated dose of 20 mg/kg/day where exposure was equivalent to the human exposure at the recommended dose of 80 mg daily (based on total AUC). Exposure at doses of 20 mg/kg and above during organogenesis caused reduced foetal weights but no adverse effects on external or visceral foetal morphology. When osimertinib was administered to pregnant female rats throughout gestation and then through early lactation, there was demonstrable exposure to osimertinib and its metabolites in suckling pups plus a reduction in pup survival and poor pup growth (at doses of 20 mg/kg and above).
CNS distribution and in vivo intracranial tumour regression: In a rat study, a single oral dose of [14C]-osimertinib was distributed to the intact brain with a maximum blood ratio of 2.2, with brain radioactivity levels being detectable out to 21 days. In an IV micro-dose PET study, [11C] osimertinib penetrated the blood-brain barrier of the intact cynomolgus monkey brain (brain to blood AUC ratio of 2.62). Osimertinib was also distributed to the intact mouse brain (brain to plasma AUC ratio 1.8-2.8) following oral dosing.
These data are consistent with observations of anti-tumour activity of osimertinib in a pre-clinical mutant-EGFR intracranial brain mouse metastasis xenograft model (PC9; exon 19 del), osimertinib (25 mg/kg/day) demonstrated significant tumour regression that was sustained during the 60 day study period, and was associated with an increase in survival of the mice compared to control animals (78% survival after 8 weeks for osimertinib compared to 11% in control group).