


 Sign Out
Sign Out

Fatal events other than those listed in Precautions as previously mentioned or in the following data that were considered possibly related to sunitinib included multisystem organ failure, disseminated intravascular coagulation, peritoneal haemorrhage, adrenal insufficiency, pneumothorax, shock, and sudden death.
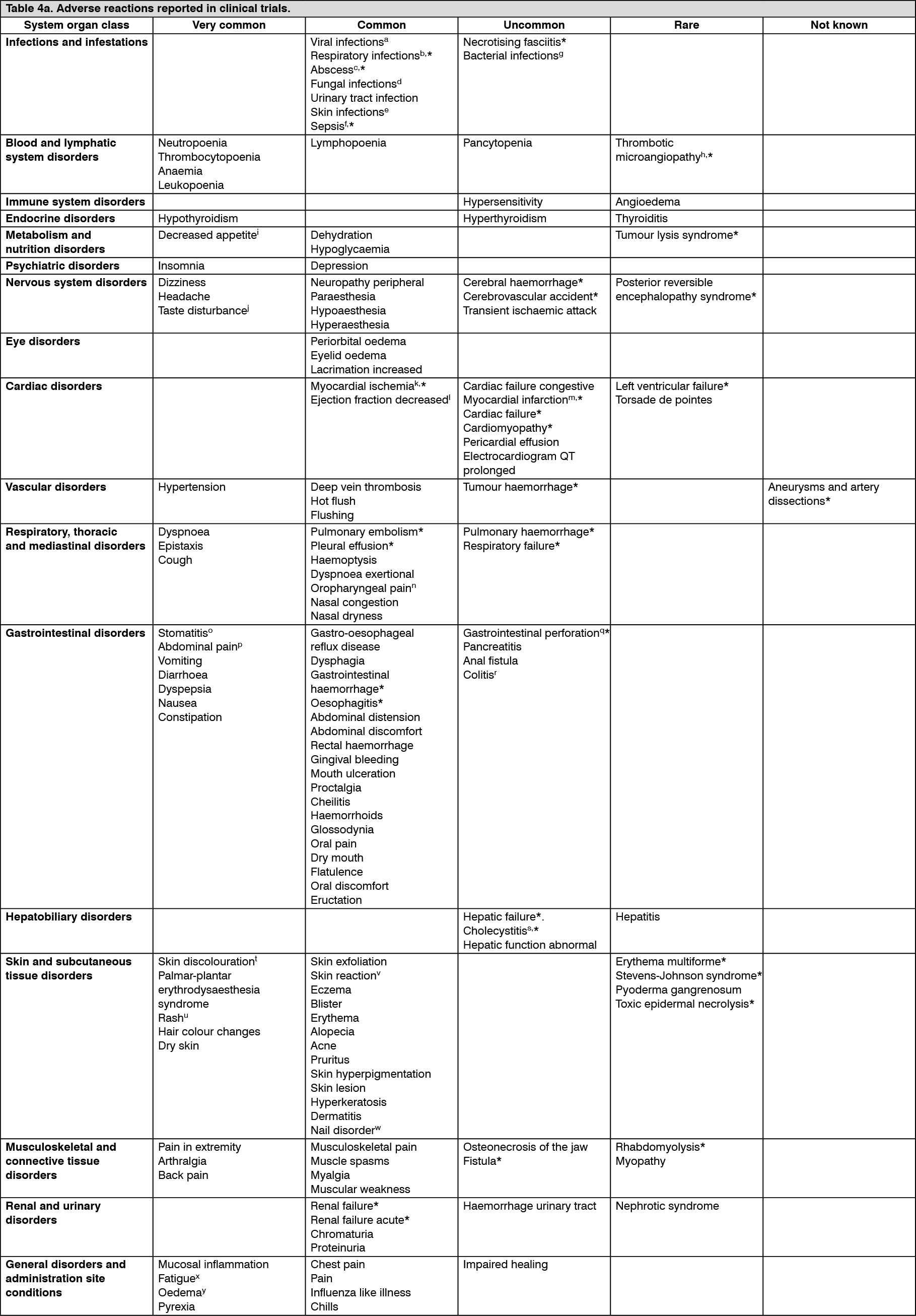
Tabulated list of adverse reactions: Adverse reactions that were reported in GIST, MRCC, and pNET patients in a pooled dataset of 7,115 patients are listed as follows, by system organ class, frequency and grade of severity (NCI-CTCAE). Post-marketing adverse reactions identified in clinical studies are also included. Within each frequency grouping, undesirable effects are presented in order of decreasing seriousness.
Frequencies are defined as: very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1,000 to <1/100), rare (≥1/10,000 to <1/1,000),very rare (<1/10,000), not known (cannot be estimated from the available data). (See Tables 4a and 4b.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image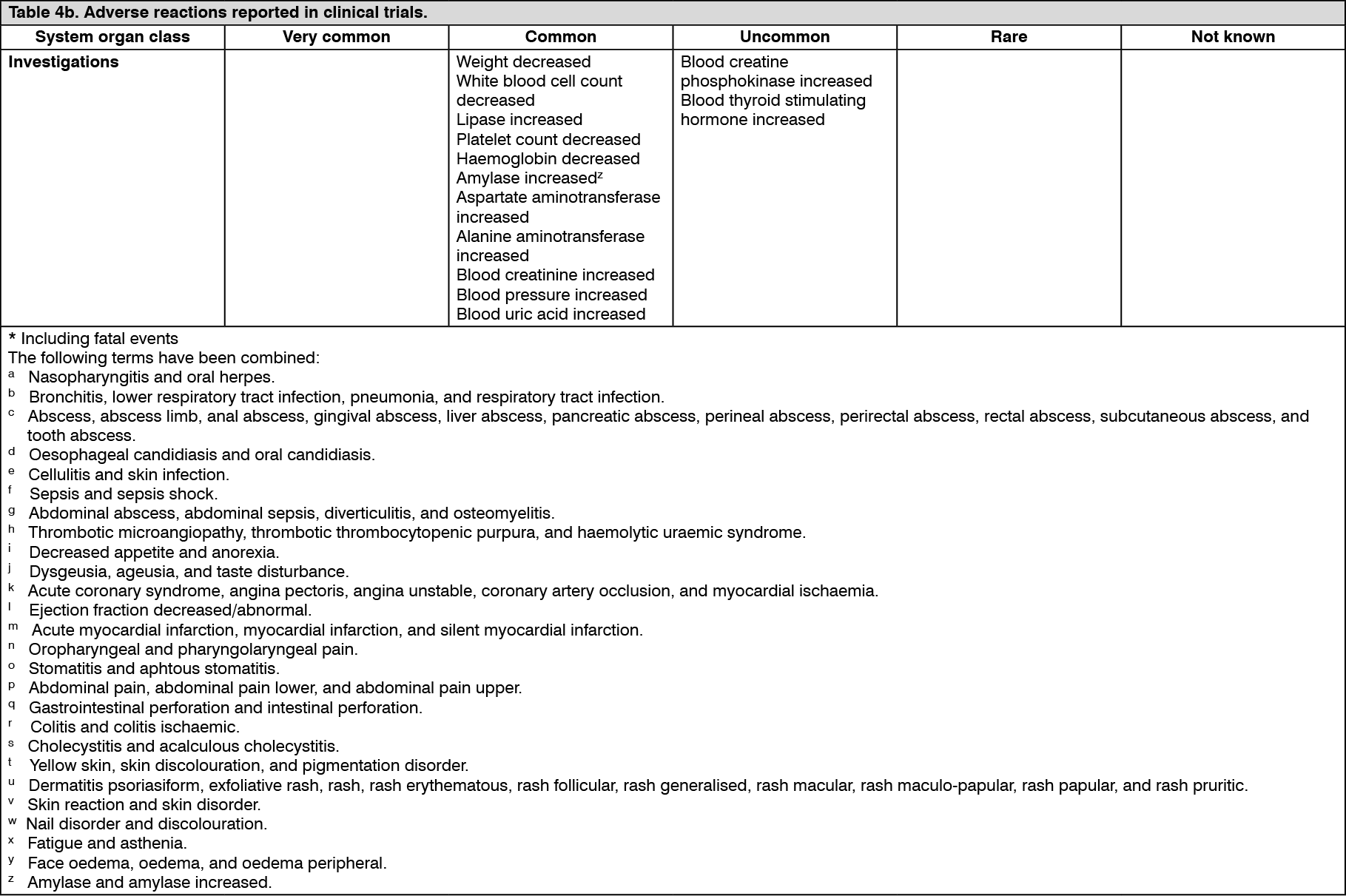 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: Infections and infestations: Cases of serious infection (with or without neutropenia), including cases with fatal outcome, have been reported. Cases of necrotising fasciitis, including of the perineum, sometimes fatal, have been reported (see also Precautions).
Blood and lymphatic system disorders: Decreased absolute neutrophil counts of Grade 3 and 4 severities, respectively, were reported in 10% and 1.7% of patients on the Phase 3 GIST study, in 16% and 1.6% of patients on the Phase 3 MRCC study, and in 13% and 2.4% of patients on the Phase 3 pNET study. Decreased platelet counts of Grade 3 and 4 severities, respectively, were reported in 3.7% and 0.4% of patients on the Phase 3 GIST study, in 8.2% and 1.1% of patients on the Phase 3 MRCC study, and in 3.7% and 1.2% of patients on the Phase 3 pNET study (see Precautions).
Bleeding events were reported in 18% of patients receiving sunitinib in a Phase 3 GIST study vs 17% of patients receiving placebo. In patients receiving sunitinib for treatment-naïve MRCC, 39% had bleeding events vs 11% of patients receiving interferon-α (IFN-α). Seventeen (4.5%) patients on sunitinib versus 5 (1.7%) patients on IFN-α experienced Grade 3 or greater bleeding events. Of patients receiving sunitinib for cytokine-refractory MRCC, 26% experienced bleeding. Bleeding events, excluding epistaxis, were reported in 21.7% of patients receiving sunitinib in the Phase 3 pNET study compared to 9.85% of patients receiving placebo (see Precautions).
In clinical trials, tumour haemorrhage was reported in approximately 2% of patients with GIST.
Immune system disorders: Hypersensitivity reactions, including angioedema, have been reported (see Precautions).
Endocrine disorders: Hypothyroidism was reported as an adverse reaction in 7 patients (4%) receiving sunitinib across the 2 cytokine-refractory MRCC studies; in 61 patients (16%) on sunitinib and 3 patients (<1%) in the IFN-α arm in the treatment-naïve MRCC study.
Additionally, thyroid-stimulating hormone (TSH) elevations were reported in 4 cytokine-refractory MRCC patients (2%). Overall, 7% of the MRCC population had either clinical or laboratory evidence of treatment-emergent hypothyroidism. Acquired hypothyroidism was noted in 6.2% of GIST patients on sunitinib versus 1% on placebo. In the Phase 3 pNET study hypothyroidism was reported in 6 patients (7.2%) receiving sunitinib and in 1 patient (1.2%) on placebo.
Thyroid function was monitored prospectively in 2 studies in patients with breast cancer; ALVOSUNI is not approved for use in breast cancer. In 1 study, hypothyroidism was reported in 15 (13.6%) patients on sunitinib and 3 (2.9%) patients on standard of care. Blood TSH increase was reported in 1 (0.9%) patient on sunitinib and no patients on standard of care. Hyperthyroidism was reported in no sunitinib-treated patients and 1 (1.0%) patient receiving standard of care. In the other study hypothyroidism was reported in a total of 31 (13%) patients on sunitinib and 2 (0.8%) patients on capecitabine. Blood TSH increase was reported in 12 (5.0%) patients on sunitinib and no patients on capecitabine. Hyperthyroidism was reported in 4 (1.7%) patients on sunitinib and no patients on capecitabine. Blood TSH decrease was reported in 3 (1.3%) patients on sunitinib and no patients on capecitabine. T4 increase was reported in 2 (0.8%) patients on sunitinib and 1 (0.4%) patient on capecitabine. T3 increase was reported in 1 (0.8%) patient on sunitinib and no patients on capecitabine. All thyroid-related events reported were Grade 1-2 (see Precautions).
Metabolism and nutrition disorders: A higher incidence rate of hypoglycaemia events was reported in patients with pNET in comparison to MRCC and GIST. Nevertheless, most of these adverse events observed in clinical studies were not considered related to study treatment (see Precautions).
Nervous system disorders: In clinical studies of sunitinib and from postmarketing surveillance, there have been few reports (<1%), some fatal, of subjects presenting with seizures and radiological evidence of RPLS. Seizures have been observed in patients with or without radiological evidence of brain metastases (see Precautions).
Cardiac disorders: In clinical trials, decreases in left ventricular ejection fraction (LVEF) of ≥20% and below the lower limit of normal were reported in approximately 2% of sunitinib-treated GIST patients, 4% of cytokine-refractory MRCC patients, and 2% of placebo-treated GIST patients. These LVEF declines do not appear to have been progressive and often improved as treatment continued. In the treatment-naïve MRCC study, 27% of patients on sunitinib and 15% of patients on IFN-α had an LVEF value below the lower limit of normal. Two patients (<1%) who received sunitinib were diagnosed with CHF.
In GIST patients 'cardiac failure', 'cardiac failure congestive', or 'left ventricular failure' were reported in 1.2% of patients treated with sunitinib and 1% of patients treated with placebo. In the pivotal Phase 3 GIST study (N =312), treatment-related fatal cardiac reactions were reported in 1% of patients on each arm of the study (i.e. sunitinib and placebo arms). In a Phase 2 study in cytokine-refractory MRCC patients, 0.9% of patients experienced treatment-related fatal myocardial infarction and in the Phase 3 study in treatment-naïve MRCC patients, 0.6% of patients on the IFN-α arm and 0% of patients on the sunitinib arm experienced fatal cardiac events. In the Phase 3 pNET study, 1 (1%) patient who received sunitinib had treatment-related fatal cardiac failure.
Vascular disorders: Hypertension: Hypertension was a very common adverse reaction reported in clinical trials. The dose of sunitinib was reduced or its administration temporarily suspended in approximately 2.7% of the patients who experienced hypertension. Sunitinib was not permanently discontinued in any of these patients. Severe hypertension (>200 mmHg systolic or 110 mmHg diastolic) was reported in 4.7% of patients with solid tumours. Hypertension was reported in approximately 33.9% of patients receiving sunitinib for treatment-naïve MRCC compared to 3.6% of patients receiving IFN-α. Severe hypertension was reported in 12% of treatment-naïve patients on sunitinib and <1% of patients on IFN-α. Hypertension was reported in 26.5% of patients receiving sunitinib in a Phase 3 pNET study, compared to 4.9% of patients receiving placebo. Severe hypertension was reported in 10% of pNET patients on sunitinib and 3% of patients on placebo.
Venous thromboembolic events: Treatment-related venous thromboembolic events were reported in approximately 1.0% of patients with solid tumours who received sunitinib on clinical trials, including GIST and RCC.
Seven patients (3%) on sunitinib and none on placebo in a Phase 3 GIST study experienced venous thromboembolic events; 5 of the 7 were Grade 3 deep venous thrombosis (DVT) and 2 were Grade 1 or 2. Four of these 7 GIST patients discontinued treatment following first observation of DVT.
Thirteen patients (3%) receiving sunitinib in the Phase 3 treatment-naïve MRCC study and 4 patients (2%) on the 2 cytokine-refractory MRCC studies had venous thromboembolic events reported. Nine of these patients had pulmonary embolisms; 1 was Grade 2 and 8 were Grade 4. Eight of these patients had DVT; 1 with Grade 1, 2 with Grade 2, 4 with Grade 3, and 1 with Grade 4. One patient with pulmonary embolism in the cytokine-refractory MRCC study experienced dose interruption.
In treatment-naïve MRCC patients receiving IFN-α, 6 (2%) venous thromboembolic events were reported; 1 patient (<1%) experienced a Grade 3 DVT and 5 patients (1%) had pulmonary embolisms, all with Grade 4.
Venous thromboembolic events were reported for 1 (1.2%) patient in the sunitinib arm and 5 (6.1%) patients in the placebo arm in the Phase 3 pNET study. Two of these patients on placebo had DVT, 1 with Grade 2 and 1 with Grade 3.
No cases with fatal outcome were reported in GIST, MRCC, and pNET registrational studies. Cases with fatal outcome have been observed in the postmarketing surveillance.
Cases of pulmonary embolism were observed in approximately 3.1% of patients with GIST and in approximately 1.2% of patients with MRCC, who received sunitinib in Phase 3 studies. No pulmonary embolism was reported for patients with pNET who received sunitinib in the Phase 3 study. Rare cases with fatal outcome have been observed in the postmarketing surveillance.
Patients who presented with pulmonary embolism within the previous 12 months were excluded from sunitinib clinical studies.
In patients who received sunitinib in Phase 3 registrational studies, pulmonary events (i.e. dyspnoea, pleural effusion, pulmonary embolism, or pulmonary oedema) were reported in approximately 17.8% of patients with GIST, in approximately 26.7% of patients with MRCC and in 12% of patients with pNET.
Approximately 22.2% of patients with solid tumours, including GIST and MRCC, who received sunitinib in clinical trials experienced pulmonary events.
Gastrointestinal disorders: Pancreatitis has been observed uncommonly (<1%) in patients receiving sunitinib for GIST or MRCC. No treatment-related pancreatitis was reported in the Phase 3 pNET study (see Precautions).
Fatal gastrointestinal bleeding was reported in 0.98% of patients receiving placebo in the GIST Phase 3 study.
Hepatobiliary disorders: Hepatic dysfunction has been reported and may include Liver Function Test abnormalities, hepatitis, or liver failure (see Precautions).
Skin and subcutaneous tissue disorders: Cases of pyoderma gangrenosum, generally reversible after discontinuation of sunitinib, have been reported (see also Precautions).
Musculoskeletal and connective tissue disorders: Cases of myopathy and/or rhabdomyolysis, some with acute renal failure, have been reported. Patients with signs or symptoms of muscle toxicity should be managed as per standard medical practice (see Precautions).
Cases of fistula formation, sometimes associated with tumour necrosis and regression, in some cases with fatal outcomes, have been reported (see Precautions).
Cases of ONJ have been reported in patients treated with ALVOSUNI, most of which occurred in patients who had identified risk factors for ONJ, in particular, exposure to intravenous bisphosphonates and/or a history of dental disease requiring invasive dental procedures (see also Precautions).
Investigations: Data from non-clinical (in vitro and in vivo) studies, at doses higher than the recommended human dose, indicated that sunitinib has the potential to inhibit the cardiac action potential repolarisation process (e.g., prolongation of QT interval).
Increases in the QTc interval to over 500 msec were reported in 0.5%, and changes from baseline in excess of 60 msec were reported in 1.1% of the 450 solid tumour patients; both of these parameters are recognised as potentially significant changes. At approximately twice therapeutic concentrations, sunitinib has been shown to prolong the QTcF interval (Fridericia corrected QT interval).
QTc interval prolongation was investigated in a trial in 24 patients, ages 20-87 years, with advanced malignancies. The results of this study demonstrated that sunitinib had an effect on QTc interval (defined as a mean placebo-adjusted change of >10 msec with a 90% confidence interval [CI] upper limit >15 msec) at therapeutic concentration (Day 3) using the within-day baseline correction method, and at greater than therapeutic concentration (Day 9) using both baseline correction methods. No patients had a QTc interval >500 msec. Although an effect on QTcF interval was observed on Day 3 at 24 hours postdose (i.e., at therapeutic plasma concentration expected after the recommended starting dose of 50 mg) with the within-day baseline correction method, the clinical significance of this finding is unclear.
Using comprehensive serial ECG assessments at times corresponding to either therapeutic or greater than therapeutic exposures, none of the patients in the evaluable or intent-to-treat (ITT) populations were observed to develop QTc interval prolongation considered as "severe" (i.e. equal to or greater than Grade 3 by Common Terminology Criteria for Adverse Events [CTCAE] version 3.0).
At therapeutic plasma concentrations, the maximum QTcF interval (Fredericia's correction) mean change from baseline was 9 msec (90% CI: 15.1msec). At approximately twice therapeutic concentrations, the maximum QTcF interval change from baseline was 15.4 msec (90% CI: 22.4 msec). Moxifloxacin (400 mg) used as a positive control showed a 5.6 msec maximum mean QTcF interval change from baseline. No subjects experienced an effect on the QTc interval greater than Grade 2 (CTCAE version 3.0) (see Precautions).
Long-term safety in MRCC: The long-term safety of sunitinib in patients with MRCC was analysed across 9 completed clinical studies conducted in the first-line, bevacizumab refractory, and cytokine-refractory treatment settings in 5,739 patients, of whom 807 (14%) were treated for ≥2 years up to 6 years. In the 807 patients who received long-term sunitinib treatment, most treatment-related adverse events (TRAEs) occurred initially in the first 6 months-1 year and then were stable or decreased in frequency over time, with the exception of hypothyroidism, which gradually increased over time, with new cases occurring over the 6-year period. Prolonged treatment with sunitinib did not appear to be associated with new types of TRAEs.
Paediatric population: The safety profile of sunitinib has been derived from a Phase 1 dose-escalation study, a Phase 2 open-label study, a Phase 1/2 single-arm study and from publications as described as follows.
A Phase 1 dose-escalation study of oral sunitinib was conducted in 35 patients comprised of 30 paediatric patients (aged 3 years to 17 years) and 5 young adult patients (aged 18 to 21 years), with refractory solid tumours, the majority of whom had a primary diagnosis of brain tumour. All study participants experienced adverse drug reactions; most of these were severe (toxicity grade ≥3) and included cardiac toxicity. The most common adverse drug reactions were gastrointestinal (GI) toxicity, neutropenia, fatigue, and ALT elevation. The risk of cardiac adverse drug reactions appeared to be higher in paediatric patients with previous exposure to cardiac irradiation or anthracycline compared to those paediatric patients without previous exposure. In these paediatric patients without previous exposure to anthracyclines or cardiac irradiation, the maximum tolerated dose (MTD) has been identified (see PHARMACOLOGY: Pharmacodynamics under Actions).
A phase 2 open-label study was conducted in 29 patients comprised of 27 paediatric patients (aged 3 years to 16 years) and 2 young adult patients (aged 18 years to 19 years) with recurrent/progressive/refractory high grade glioma (HGG) or ependymoma. There were no Grade 5 adverse reactions in either group. The most common (≥10%) treatment-related adverse events were neutrophil count decreased (6 [20.7%] patients) and haemorrhage intracranial (3[10.3%] patients).
A Phase 1/2 single-arm, study was conducted in 6 paediatric patients (aged 13 years to 16 years) with advanced unresectable GIST. The most frequent adverse drug reactions were diarrhoea, nausea, WBC count decreased, neutropenia, and headache in 3 (50.0%) patients each, primarily Grade 1 or 2 in severity. Four out of 6 patients (66.7%) experienced Grade 3-4 treatment-related adverse events (Grade 3 hypophosphataemia, neutropenia, and thrombocytopenia in 1 patient each and a Grade 4 neutropenia in 1 patient). There were no serious adverse events (SAEs) or Grade 5 adverse drug reactions reported in this study. In both the clinical study and the publications, the safety profile was consistent with the known safety profile in adults.
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the national reporting system.
View ADR Monitoring Form