


 Sign Out
Sign Out



Clinical Trials Experience: Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
MRD-positive B-cell Precursor ALL: The safety of BLINCYTO in patients with MRD-positive B-cell precursor ALL was evaluated in two single-arm clinical studies in which 137 patients were treated with BLINCYTO. The median age of the study population was 45 years (range: 18 to 77 years).
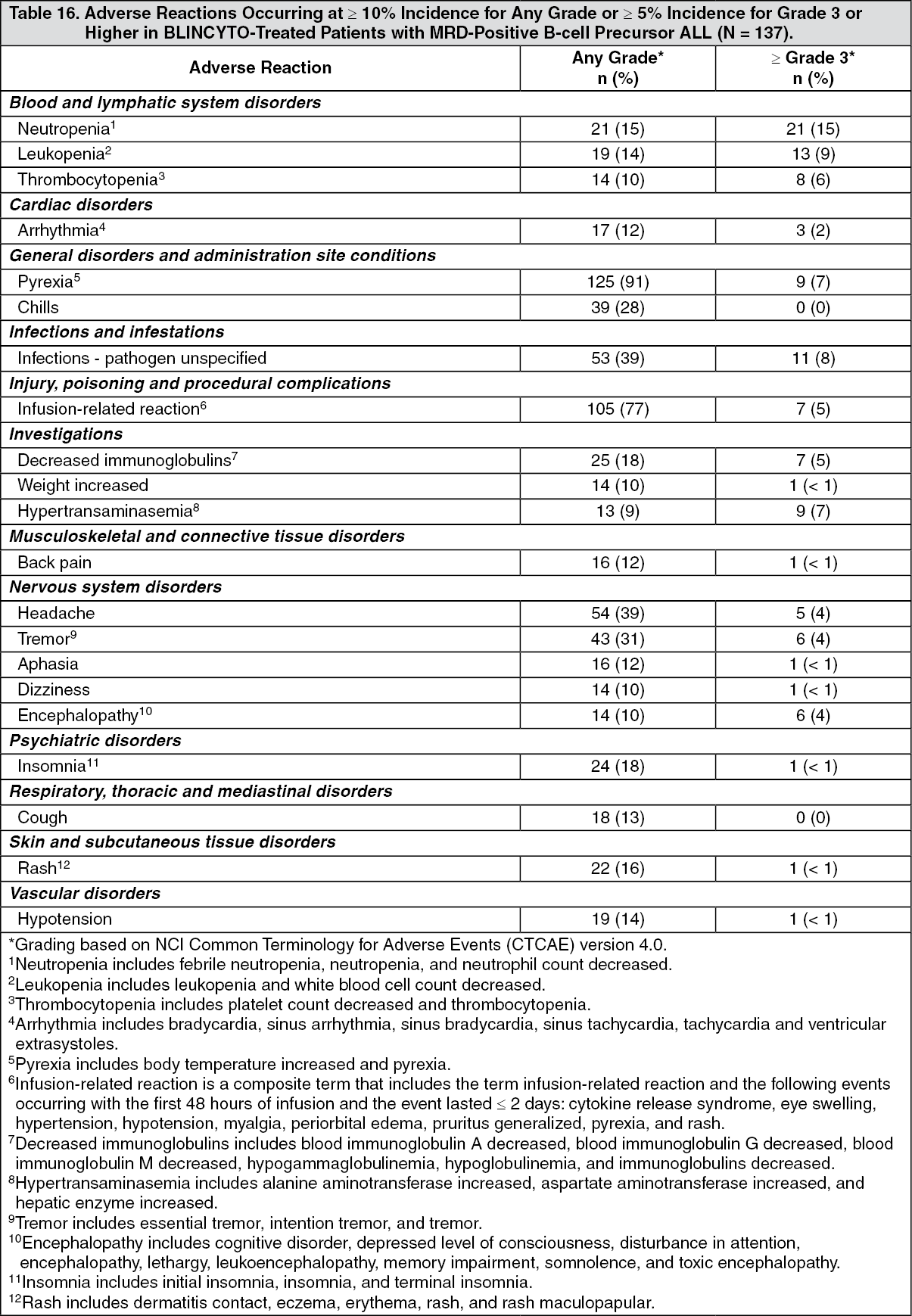
The most common adverse reactions (≥ 20%) were pyrexia, infusion-related reactions, headache, infections (pathogen unspecified), tremor, and chills. Serious adverse reactions were reported in 61% of patients. The most common serious adverse reactions (≥ 2%) included pyrexia, tremor, encephalopathy, aphasia, lymphopenia, neutropenia, overdose, device related infection, seizure, and staphylococcal infection. Adverse reactions of Grade 3 or higher were reported in 64% of patients. Discontinuation of therapy due to adverse reactions occurred in 17% of patients; neurologic events were the most frequently reported reasons for discontinuation. There were 2 fatal adverse events that occurred within 30 days of the end of BLINCYTO treatment (atypical pneumonia and subdural hemorrhage).
Table 16 summarizes the adverse reactions occurring at a ≥ 10% incidence for any grade or ≥ 5% incidence for Grade 3 or higher. (See Table 16.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAdditional adverse reactions in patients with MRD-positive ALL that did not meet the threshold criteria for inclusion in Table 16 were: Blood and lymphatic system disorders: anemia.
General disorders and administration site conditions: edema peripheral, pain, and chest pain (includes chest pain and musculoskeletal chest pain).
Hepatobiliary disorders: blood bilirubin increased.
Immune system disorders: hypersensitivity and cytokine release syndrome.
Infections and infestations: viral infectious disorders, bacterial infectious disorders, and fungal infectious disorders.
Injury, poisoning and procedural complications: medication error and overdose (includes overdose and accidental overdose).
Investigations: blood alkaline phosphatase increased.
Musculoskeletal and connective tissue disorders: pain in extremity and bone pain.
Nervous system disorders: seizure (includes seizure and generalized tonic-clonic seizure), speech disorder, and hypoesthesia.
Psychiatric disorders: confusional state, disorientation, and depression.
Respiratory, thoracic and mediastinal disorders: dyspnea and productive cough.
Vascular disorders: hypertension (includes blood pressure increased and hypertension) flushing (includes flushing and hot flush), and capillary leak syndrome.
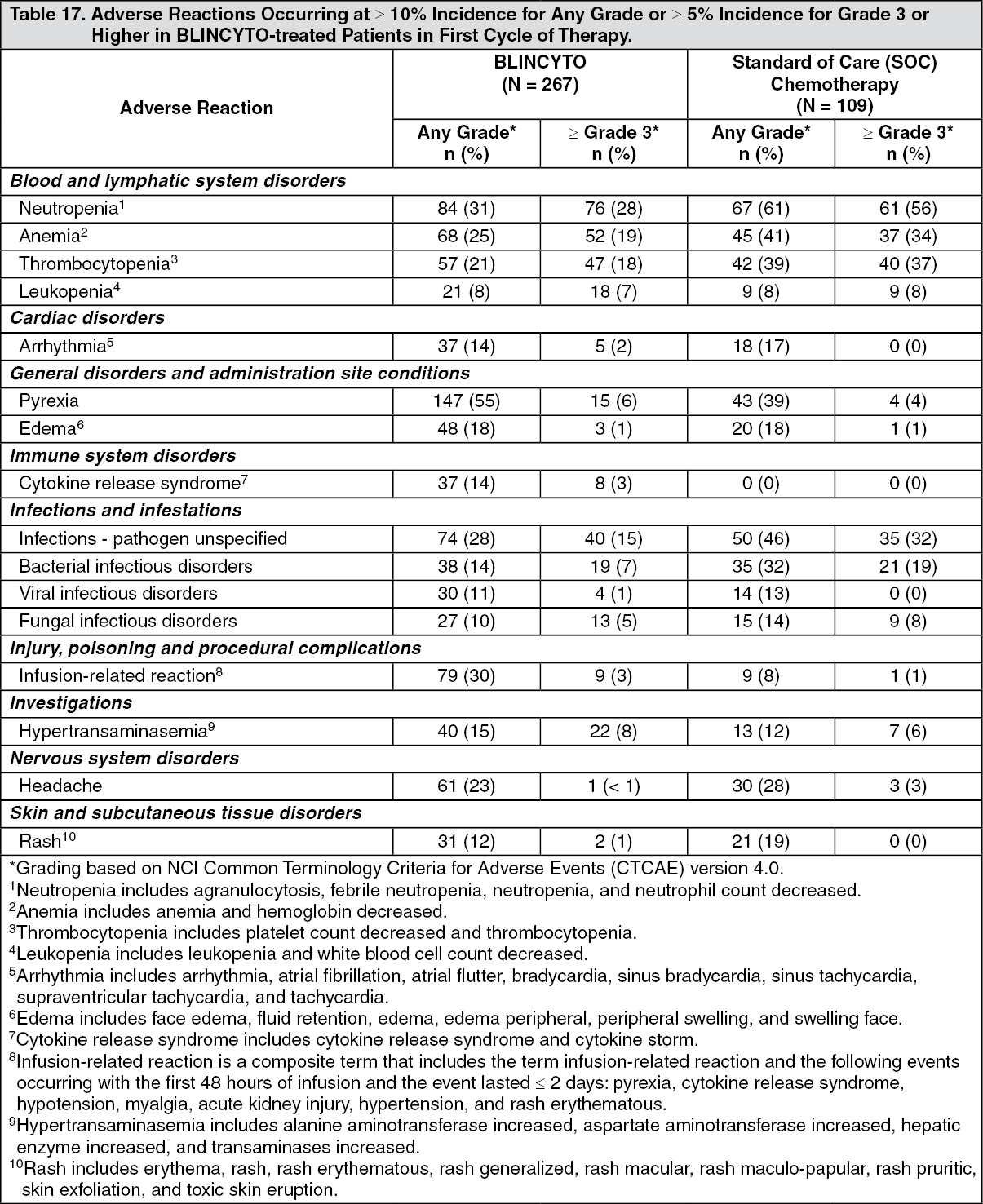
Philadelphia Chromosome-negative Relapsed or Refractory B-cell Precursor ALL: The safety data described as follows reflect exposure to BLINCYTO in a randomized, open-label, active-controlled clinical study (TOWER Study) in which 376 patients with Philadelphia chromosome-negative relapsed or refractory B-cell precursor ALL were treated with BLINCYTO (n = 267) or standard of care (SOC) chemotherapy (n = 109). The median age of BLINCYTO-treated patients was 37 years (range: 18 to 80 years), 60% were male, 84% were White, 7% Asian, 2% were Black or African American, 2% were American Indian or Alaska Native, and 5% were Multiple/Other.
The most common adverse reactions (≥ 20%) in the BLINCYTO arm were infections (bacterial and pathogen unspecified), pyrexia, headache, infusion-related reactions, anemia, febrile neutropenia, thrombocytopenia, and neutropenia. Serious adverse reactions were reported in 62% of patients. The most common serious adverse reactions (≥ 2%) included febrile neutropenia, pyrexia, sepsis, pneumonia, overdose, septic shock, CRS, bacterial sepsis, device related infection, and bacteremia. Adverse reactions of Grade 3 or higher were reported in 87% of patients. Discontinuation of therapy due to adverse reactions occurred in 12% of patients treated with BLINCYTO; neurologic events and infections were the most frequently reported reasons for discontinuation of treatment due to an adverse reaction. Fatal adverse events occurred in 16% of patients. The majority of the fatal events were infections.
The adverse reactions occurring at a ≥ 10% incidence for any grade or ≥ 5% incidence for Grade 3 or higher in the BLINCYTO-treated patients in first cycle of therapy are summarized in Table 17. (See Table 17.)
 Click on icon to see table/diagram/image
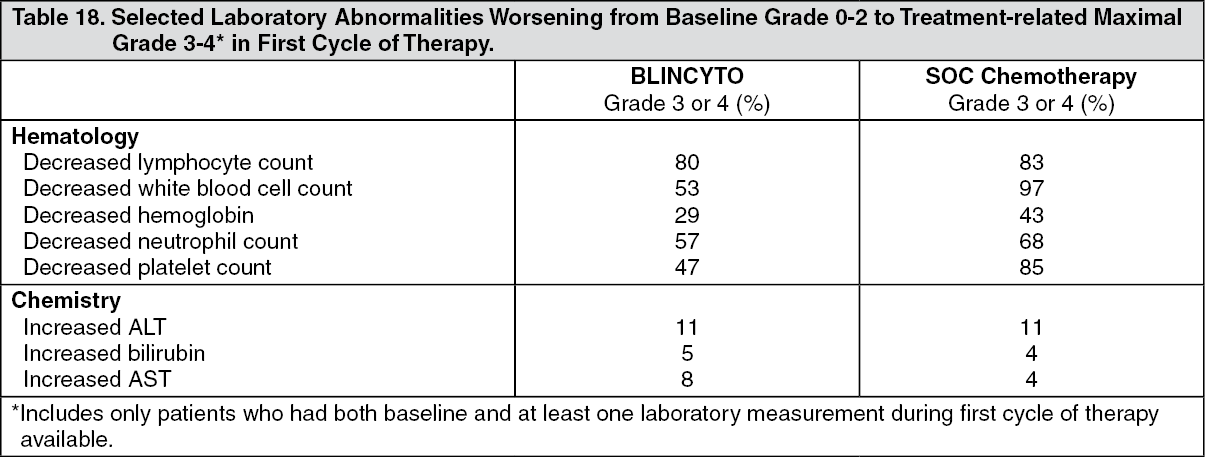
Click on icon to see table/diagram/imageSelected laboratory abnormalities worsening from baseline Grade 0-2 to treatment-related maximal Grade 3-4 in first cycle of therapy are shown in Table 18. (See Table 18.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageRelapsed or Refractory B-cell Precursor ALL: Other important adverse reactions from pooled relapsed or refractory B-cell precursor ALL studies were: Blood and lymphatic system disorders: lymphadenopathy, hematophagic histiocytosis, and leukocytosis (includes leukocytosis and white blood cell count increased).
General disorders and administration site conditions: chills, chest pain (includes chest discomfort, chest pain, musculoskeletal chest pain, and non-cardiac chest pain), pain, body temperature increased, hyperthermia, and systemic inflammatory response syndrome.
Hepatobiliary disorders: hyperbilirubinemia (includes blood bilirubin increased and hyperbilirubinemia).
Immune system disorders: hypersensitivity (includes hypersensitivity, anaphylactic reaction, angioedema, dermatitis allergic, drug eruption, drug hypersensitivity, erythema multiforme, and urticaria).
Injury, poisoning and procedural complications: medication error and overdose (includes overdose, medication error, and accidental overdose)
Investigations: weight increased, decreased immunoglobulins (includes immunoglobulins decreased, blood immunoglobulin A decreased, blood immunoglobulin G decreased, blood immunoglobulin M decreased, and hypogammaglobulinemia), blood alkaline phosphatase increased, and hypertransaminasemia.
Metabolism and nutrition disorders: tumor lysis syndrome.
Musculoskeletal and connective tissue disorders: back pain, bone pain, and pain in extremity.
Nervous system disorders: tremor (resting tremor, intention tremor, essential tremor, and tremor), altered state of consciousness (includes altered state of consciousness, depressed level of consciousness, disturbance in attention, lethargy, mental status changes, stupor, and somnolence), dizziness, memory impairment, seizure (includes seizure, and atonic seizure), aphasia, cognitive disorder, speech disorder, hypoesthesia, encephalopathy, and cranial nerve disorders (trigeminal neuralgia, trigeminal nerve disorder, sixth nerve paralysis, cranial nerve disorder, facial nerve disorder, and facial paresis).
Psychiatric disorders: insomnia, disorientation, confusional state, and depression (includes depressed mood, depression, suicidal ideation, and completed suicide)
Respiratory, thoracic and mediastinal disorders: dyspnea (includes acute respiratory failure, dyspnea, dyspnea exertional, respiratory failure, respiratory distress, bronchospasm, bronchial hyperreactivity, tachypnea, and wheezing), cough, and productive cough.
Vascular disorders: hypotension (includes blood pressure decreased, hypotension, hypovolemic shock, and circulatory collapse), hypertension (includes blood pressure increased, hypertension, and hypertensive crisis), flushing (includes flushing and hot flush), and capillary leak syndrome.
Postmarketing Experience: The following adverse reactions have been identified during post approval use of BLINCYTO. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Fatal pancreatitis has been reported in patients receiving BLINCYTO in combination with dexamethasone [see Pancreatitis under Precautions].
Immunogenicity: As with all therapeutic proteins, there is potential for immunogenicity. The immunogenicity of BLINCYTO has been evaluated using either an electrochemiluminescence detection technology (ECL) or an enzyme-linked immunosorbent assay (ELISA) screening immunoassay for the detection of binding anti-blinatumomab antibodies. For patients whose sera tested positive in the screening immunoassay, an in vitro biological assay was performed to detect neutralizing antibodies.
In clinical studies, less than 2% of patients treated with BLINCYTO tested positive for binding anti-blinatumomab antibodies. Of patients who developed anti-blinatumomab antibodies, 7 out of 9 (78%) had in vitro neutralizing activity. Anti-blinatumomab antibody formation may affect pharmacokinetics of BLINCYTO.
The detection of anti-blinatumomab antibody formation is highly dependent on the sensitivity and specificity of the assay. Additionally, the observed incidence of antibody (including neutralizing antibody) positivity in an assay may be influenced by several factors, including assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of the incidence of antibodies to blinatumomab with the incidence of antibodies to other products may be misleading.
View ADR Monitoring Form