


 Sign Out
Sign Out



Pharmacodynamics: During the continuous intravenous infusion over 4 weeks, the pharmacodynamic response was characterized by T-cell activation and initial redistribution, reduction in peripheral B cells, and transient cytokine elevation.
Peripheral T-cell redistribution (i.e., T-cell adhesion to blood vessel endothelium and/or transmigration into tissue) occurred after start of BLINCYTO infusion or dose escalation. T-cell counts initially declined within 1 to 2 days and then returned to baseline levels within 7 to 14 days in the majority of patients. Increase of T-cell counts above baseline (T-cell expansion) was observed in few patients.
Peripheral B-cell counts decreased to less than or equal to 10 cells/microliter during the first treatment cycle at doses ≥ 5 mcg/m2/day or ≥ 9 mcg/day in the majority of patients. No recovery of peripheral B-cell counts was observed during the 2-week BLINCYTO-free period between treatment cycles. Incomplete depletion of B cells occurred at doses of 0.5 mcg/m2/day and 1.5 mcg/m2/day and in a few patients at higher doses.
Cytokines including IL-2, IL-4, IL-6, IL-8, IL-10, IL-12, TNF-α, and IFN-γ were measured, and IL-6, IL-10, and IFN-γ were elevated. The highest elevation of cytokines was observed in the first 2 days following start of BLINCYTO infusion. The elevated cytokine levels returned to baseline within 24 to 48 hours during the infusion. In subsequent treatment cycles, cytokine elevation occurred in fewer patients with lesser intensity compared to the initial 48 hours of the first treatment cycle.
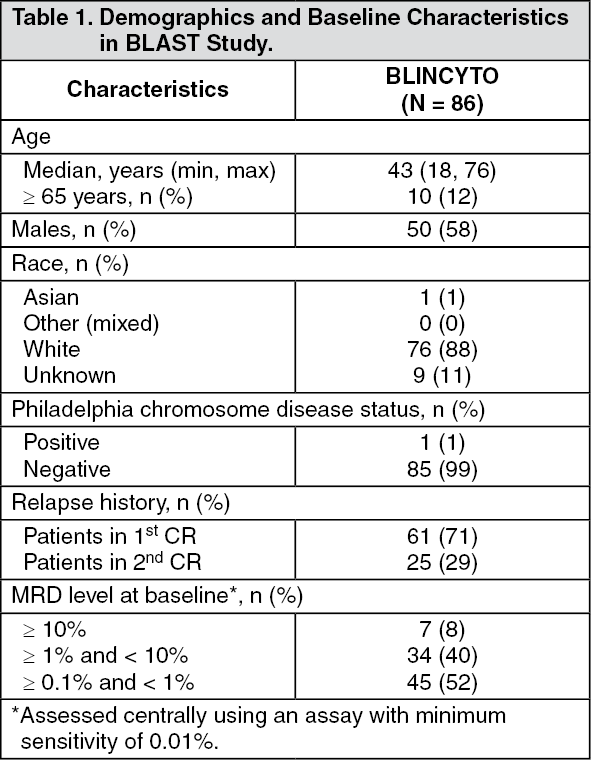
Clinical Studies: MRD-positive B-cell Precursor ALL: BLAST Study: The efficacy of BLINCYTO was evaluated in an open-label, multicenter, single-arm study (BLAST Study) [NCT01207388] that included patients who were ≥ 18 years of age, had received at least 3 chemotherapy blocks of standard ALL therapy, were in hematologic complete remission (defined as < 5% blasts in bone marrow, absolute neutrophil count > 1 Gi/L, platelets > 100 Gi/L) and had MRD at a level of ≥ 0.1% using an assay with a minimum sensitivity of 0.01%. BLINCYTO was administered at a constant dose of 15 mcg/m2/day (equivalent to the recommended dosage of 28 mcg/day) intravenously for all treatment cycles. Patients received up to 4 cycles of treatment. Dose adjustment was possible in case of adverse events.
The treated population included 86 patients in first or second hematologic complete remission (CR1 or CR2). The demographics and baseline characteristics are shown in Table 1. The median number of treatment cycles was 2 (range: 1 to 4). Following treatment with BLINCYTO, 45 out of 61 (73.8%) patients in CR1 and 14 out of 25 (56.0%) patients in CR2 underwent allogeneic hematopoietic stem cell transplantation in continuous hematologic complete remission. (See Table 1.)
 Click on icon to see table/diagram/image
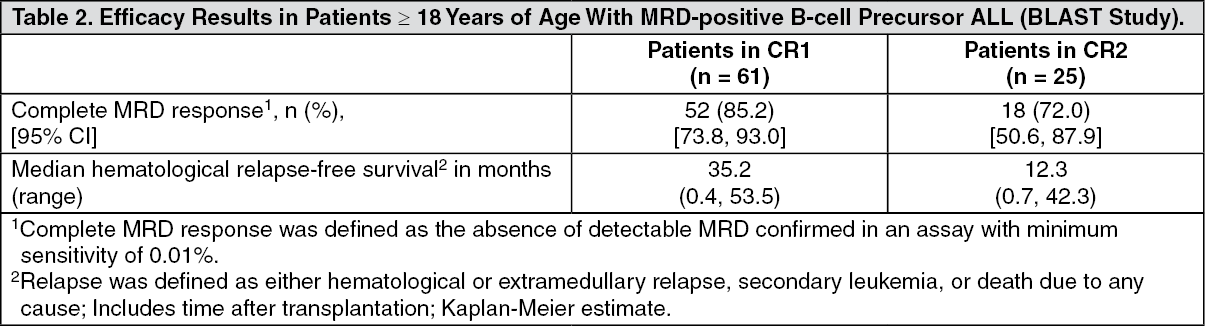
Click on icon to see table/diagram/imageEfficacy was based on achievement of undetectable MRD within one cycle of BLINCYTO treatment and hematological relapse-free survival (RFS). The assay used to assess MRD response had a sensitivity of 0.01% for 6 patients and ≤ 0.005% for 80 patients. Overall, undetectable MRD was achieved by 70 patients (81.4%: 95% CI: 71.6%, 89.0%). The median hematological RFS was 22.3 months. Table 2 shows the MRD response and hematological RFS by remission number. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageUndetectable MRD was achieved by 65 of 80 patients (81.3%: 95% CI: 71.0%, 89.1%) with an assay sensitivity of at least 0.005%. The estimated median hematological RFS among the 80 patients using the higher sensitivity assay was 24.2 months (95% CI: 17.9, NE).
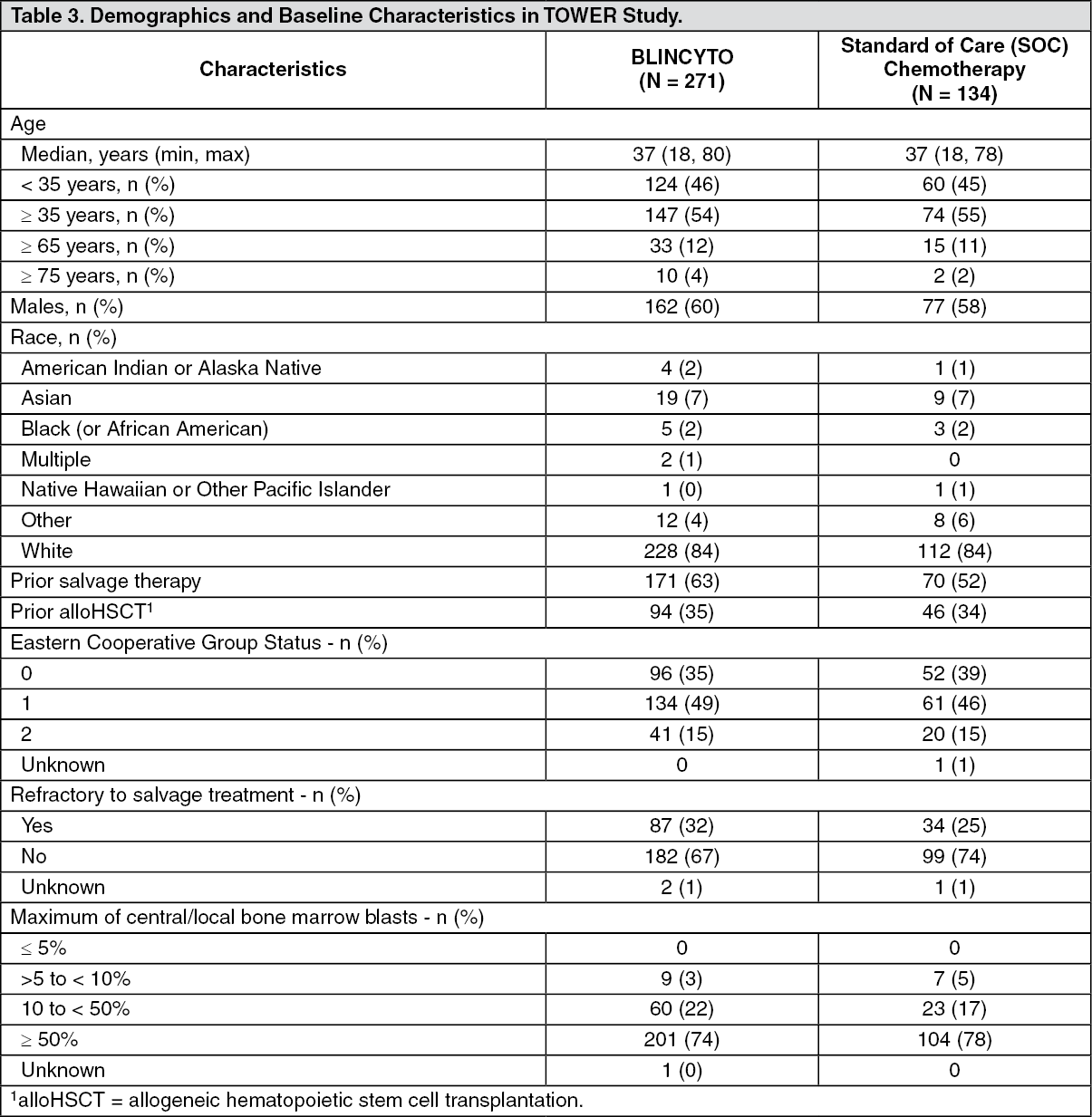
Relapsed/Refractory B-cell Precursor ALL: TOWER Study: The efficacy of BLINCYTO was compared to standard of care (SOC) chemotherapy in a randomized, open-label, multicenter study (TOWER Study) [NCT02013167]. Eligible patients were ≥ 18 years of age with relapsed or refractory B-cell precursor ALL [> 5% blasts in the bone marrow and refractory to primary induction therapy or refractory to last therapy, untreated first relapse with first remission duration < 12 months, untreated second or later relapse, or relapse at any time after allogeneic hematopoietic stem cell transplantation (alloHSCT)]. BLINCYTO was administered at 9 mcg/day on Days 1-7 and 28 mcg/day on Days 8-28 for Cycle 1, and 28 mcg/day on Days 1-28 for Cycles 2-5 in 42-day cycles and for Cycles 6-9 in 84-day cycles. Dose adjustment was possible in case of adverse events. SOC chemotherapy included fludarabine, cytarabine arabinoside, and granulocyte colony-stimulating factor (FLAG); high-dose cytarabine arabinoside (HiDAC); high-dose methotrexate- (HDMTX) based combination; or clofarabine/clofarabine-based regimens.
There were 405 patients randomized 2:1 to receive BLINCYTO or investigator-selected SOC chemotherapy. Randomization was stratified by age (< 35 years vs. ≥ 35 years of age), prior salvage therapy (yes vs. no), and prior alloHSCT (yes vs. no) as assessed at the time of consent. The demographics and baseline characteristics were well-balanced between the two arms (see Table 3).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageOf the 271 patients randomized to the BLINCYTO arm, 267 patients received BLINCYTO treatment. The median number of treatment cycles was two (range: 1 to 9 cycles); 267 (99%) received Cycles 1-2 (induction), 86 (32%) received Cycles 3-5 (consolidation), and 27 (10%) received Cycles 6-9 (continued therapy). Of the 134 patients on the SOC arm, 25 dropped out prior to start of study treatment, and 109 patients received a median of 1 treatment cycle (range: 1 to 4 cycles).
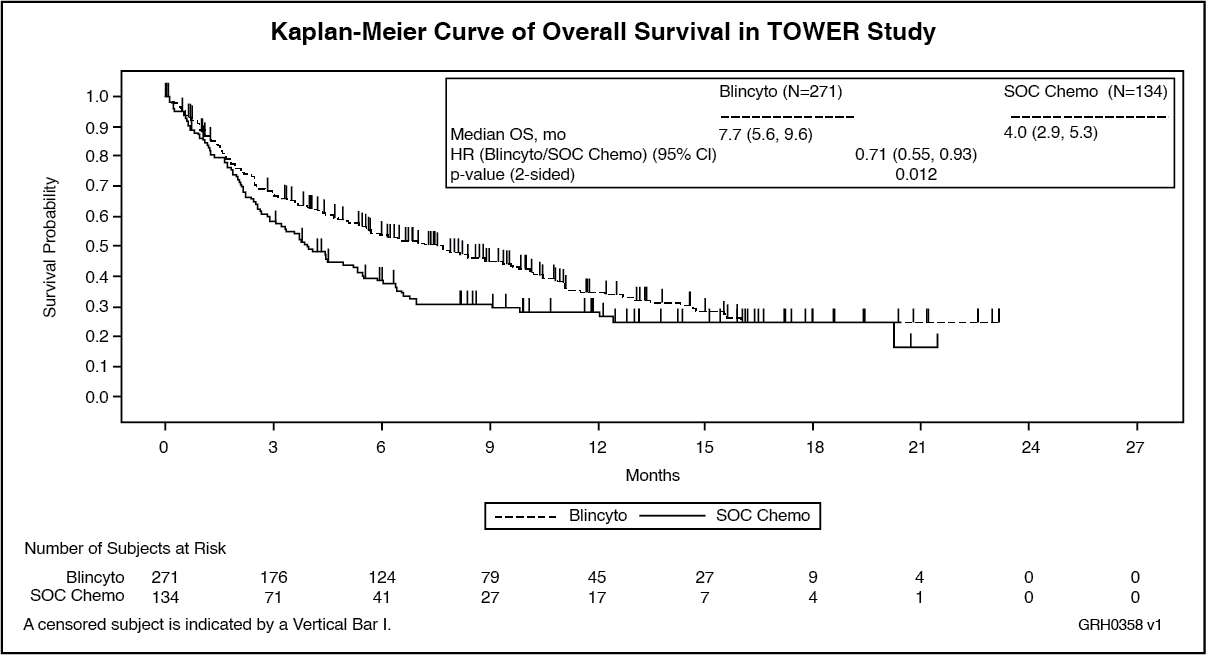
The determination of efficacy was based on overall survival (OS). The study demonstrated statistically significant improvement in OS for patients treated with BLINCYTO as compared to SOC chemotherapy.
See Figure and Table 4 as follows for efficacy results from the TOWER Study. (See Figure and Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image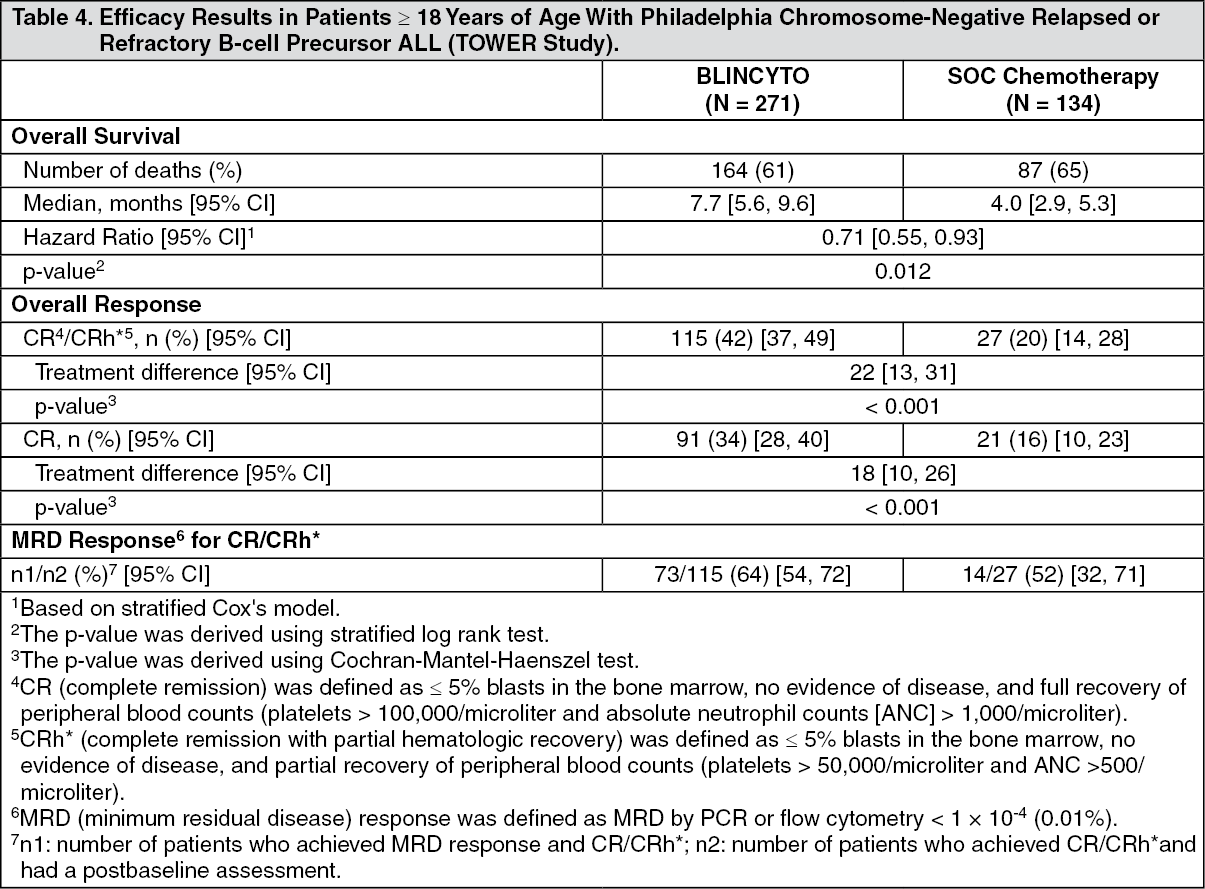 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageHealth Related Quality of Life: Health Related Quality of Life (HRQoL) reported by patients were measured using the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire - Core 30 (EORTC QLQ-C30). In a post-hoc sensitivity analysis, compared to SOC, BLINCYTO consistently delayed the time to clinically meaningful deterioration of HRQoL (≥ 10 point worsening from baseline) for global health status [median BLINCYTO vs. SOC: 8.1 months vs. 1.0 month; HR = 0.60 (95% CI = 0.42, 0.85)], functional scales, symptom scales and individual items.
Study MT103-211: Study MT103-211 [NCT01466179] was an open-label, multicenter, single-arm study. Eligible patients were ≥ 18 years of age with Philadelphia chromosome-negative relapsed or refractory B-cell precursor ALL (relapsed with first remission duration of ≤ 12 months in first salvage or relapsed or refractory after first salvage therapy or relapsed within 12 months of alloHSCT, and had ≥ 10% blasts in bone marrow).
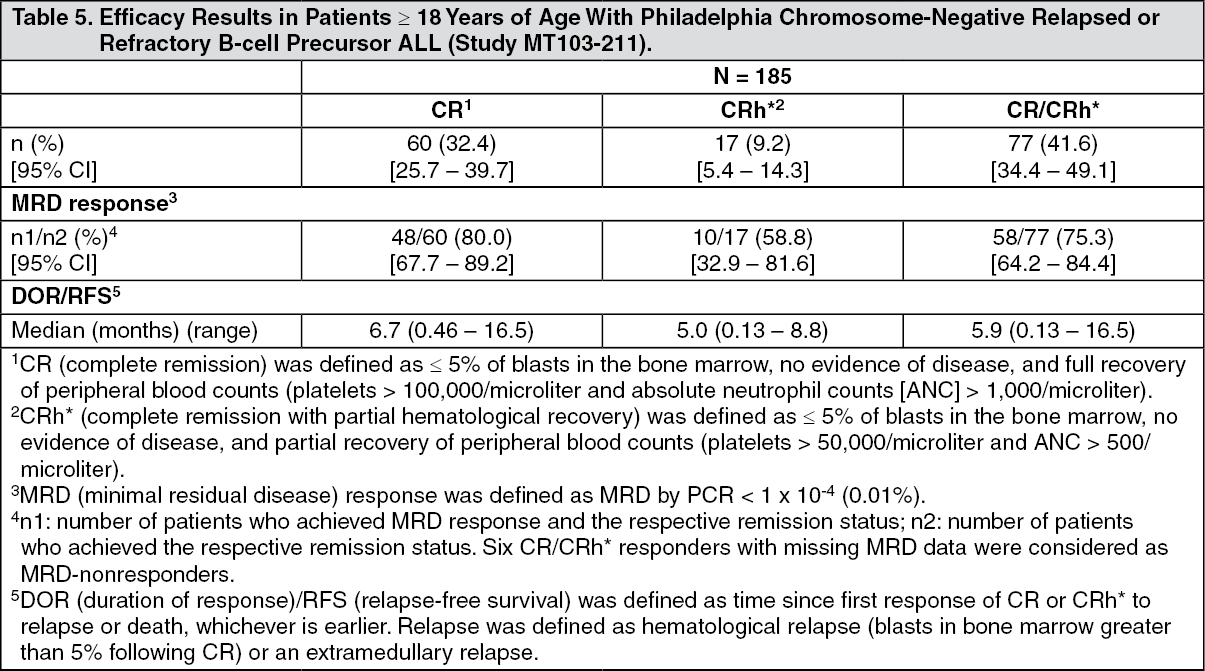
BLINCYTO was administered as a continuous intravenous infusion. The recommended dose for this study was determined to be 9 mcg/day on Days 1-7 and 28 mcg/day on Days 8-28 for Cycle 1, and 28 mcg/day on Days 1-28 for subsequent cycles. Dose adjustment was possible in case of adverse events. The treated population included 185 patients who received at least 1 infusion of BLINCYTO; the median number of treatment cycles was 2 (range: 1 to 5). Patients who responded to BLINCYTO but later relapsed had the option to be retreated with BLINCYTO. Among treated patients, the median age was 39 years (range: 18 to 79 years), 63 out of 185 (34.1%) had undergone HSCT prior to receiving BLINCYTO, and 32 out of 185 (17.3%) had received more than 2 prior salvage therapies.
Efficacy was based on the complete remission (CR) rate, duration of CR, and proportion of patients with an MRD-negative CR/CR with partial hematological recovery (CR/CRh*) within 2 cycles of treatment with BLINCYTO. Table 5 shows the efficacy results from this study. The HSCT rate among those who achieved CR/CRh* was 39% (30 out of 77). (See Table 5.)
 Click on icon to see table/diagram/image
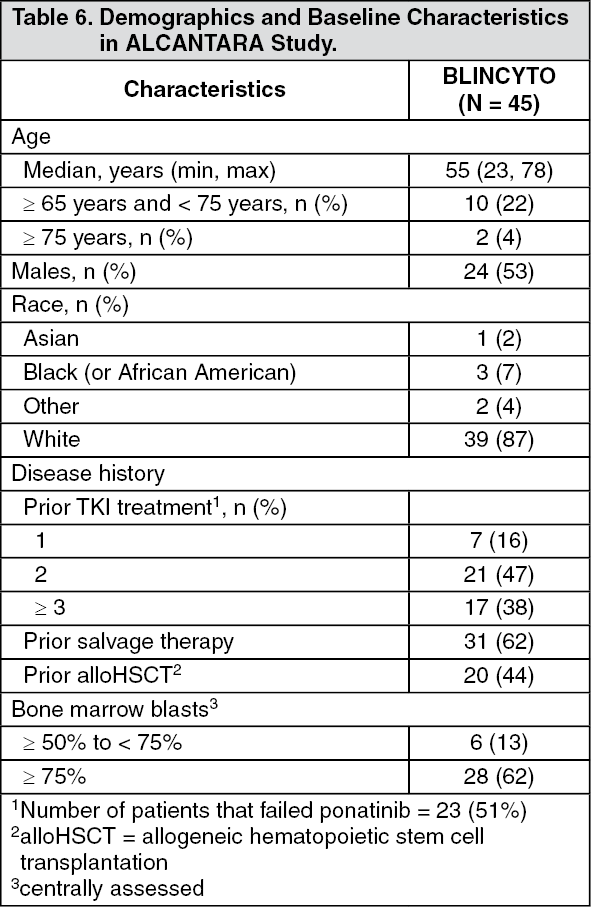
Click on icon to see table/diagram/imageALCANTARA Study: The efficacy of BLINCYTO for treatment of Philadelphia chromosome-positive B-cell precursor ALL was evaluated in an open-label, multicenter, single-arm study (ALCANTARA Study) [NCT02000427]. Eligible patients were ≥ 18 years of age with Philadelphia chromosome-positive B-cell precursor ALL, relapsed or refractory to at least 1 second generation or later tyrosine kinase inhibitor (TKI), or intolerant to second generation TKI, and intolerant or refractory to imatinib mesylate.
BLINCYTO was administered at 9 mcg/day on Days 1-7 and 28 mcg/day on Days 8-28 for Cycle 1, and 28 mcg/day on Days 1-28 for subsequent cycles. Dose adjustment was possible in case of adverse events.
The treated population included 45 patients who received at least one infusion of BLINCYTO; the median number of treatment cycles was 2 (range: 1 to 5). The demographics and baseline characteristics are shown in Table 6. (See Table 6.)
 Click on icon to see table/diagram/image
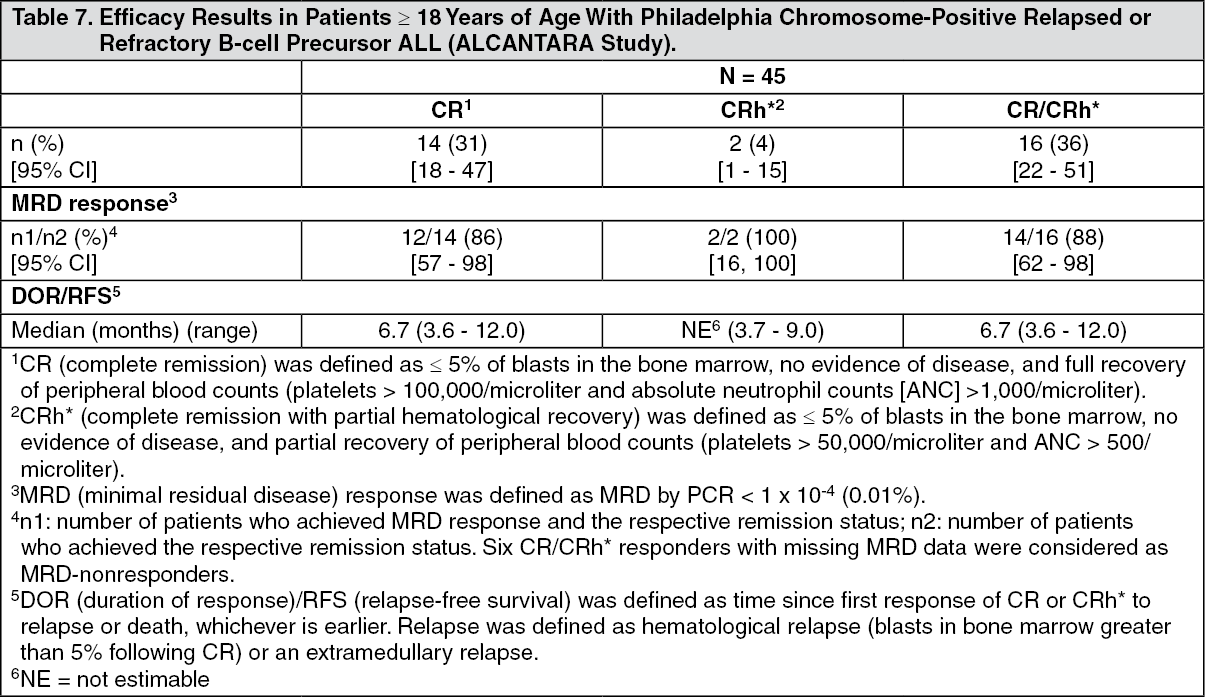
Click on icon to see table/diagram/imageEfficacy was based on the complete remission (CR) rate, duration of CR, and proportion of patients with an MRD-negative CR/CR with partial hematological recovery (CR/CRh*) within 2 cycles of treatment with BLINCYTO. Table 7 shows the efficacy results from ALCANTARA Study. Five of the 16 responding (31%) patients underwent allogeneic HSCT in CR/CRh* induced with BLINCYTO. There were 10 patients with documented T315I mutation; four achieved CR within 2 cycles of treatment with BLINCYTO. (See Table 7.)
 Click on icon to see table/diagram/image
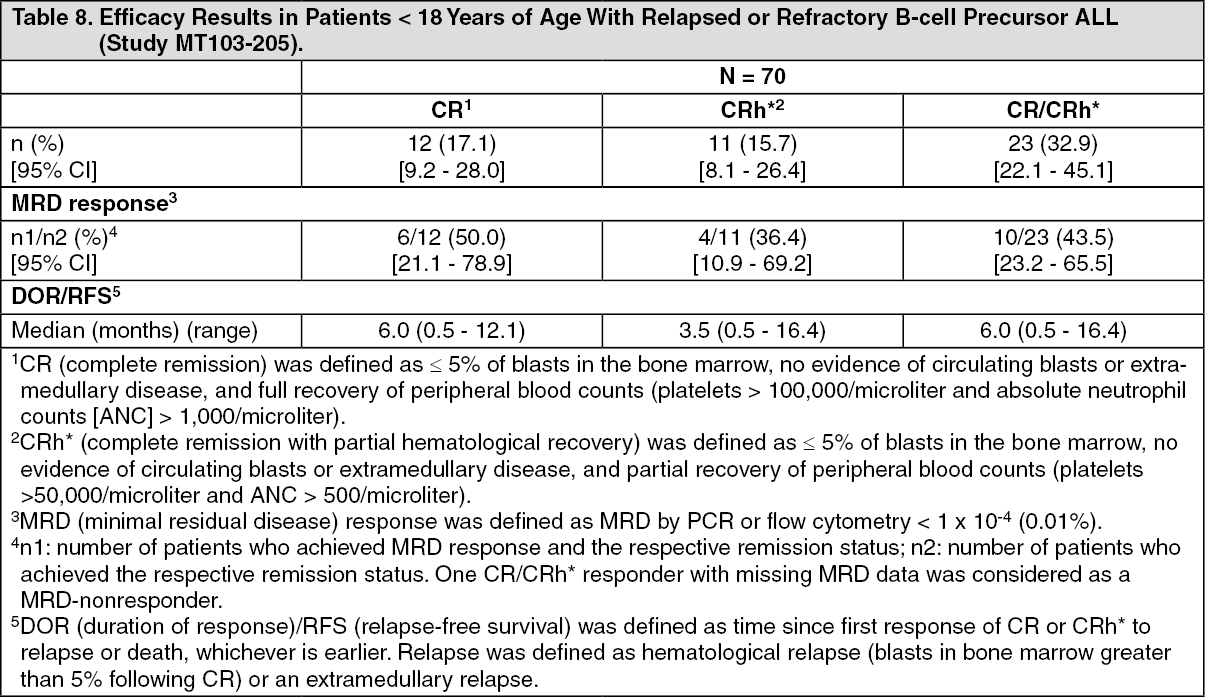
Click on icon to see table/diagram/imageStudy MT103-205: Study MT103-205 [NCT01471782] was an open-label, multicenter, single-arm study in pediatric patients with relapsed or refractory B-cell precursor ALL (second or later bone marrow relapse, any marrow relapse after allogeneic HSCT, or refractory to other treatments, and had > 25% blasts in bone marrow). BLINCYTO was administered at 5 mcg/m2/day on Days 1-7 and 15 mcg/m2/day on Days 8-28 for Cycle 1, and 15 mcg/m2/day on Days 1-28 for subsequent cycles. Dose adjustment was possible in case of adverse events. Patients who responded to BLINCYTO but later relapsed had the option to be retreated with BLINCYTO.
Among the 70 treated patients, the median age was 8 years (range: 7 months to 17 years), 40 out of 70 (57.1%) had undergone allogeneic HSCT prior to receiving BLINCYTO, and 39 out of 70 (55.7%) had refractory disease. The median number of treatment cycles was 1 (range: 1 to 5).
Twenty-three out of 70 (32.9%) patients achieved CR/CRh* within the first 2 treatment cycles with 17 out of 23 (73.9%) occurring within Cycle 1 of treatment. See Table 8 for the efficacy results from the study. The HSCT rate among those who achieved CR/CRh* was 48% (11 out of 23). (See Table 8.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePharmacokinetics: The pharmacokinetics of blinatumomab appear linear over a dose range from 5 to 90 mcg/m2/day (approximately equivalent to 9 to 162 mcg/day) in adult patients. Following continuous intravenous infusion, the steady-state serum concentration (Css) was achieved within a day and remained stable over time. The increase in mean Css values was approximately proportional to the dose in the range tested. At the clinical doses of 9 mcg/day and 28 mcg/day for the treatment of relapsed or refractory ALL, the mean (SD) Css was 228 (356) pg/mL and 616 (537) pg/mL, respectively.
Distribution: The estimated mean (SD) volume of distribution based on terminal phase (Vz) was 4.35 (2.45) L with continuous intravenous infusion of blinatumomab.
Metabolism: The metabolic pathway of blinatumomab has not been characterized. Like other protein therapeutics, BLINCYTO is expected to be degraded into small peptides and amino acids via catabolic pathways.
Elimination: The estimated mean (SD) systemic clearance with continuous intravenous infusion in patients receiving blinatumomab in clinical studies was 3.11 (2.98) L/hour. The mean (SD) half-life was 2.10 (1.41) hours. Negligible amounts of blinatumomab were excreted in the urine at the tested clinical doses.
Gender, Age, and Body Surface Area: Results of population pharmacokinetic analyses indicate that age (0.62 to 80 years of age) and gender do not influence the pharmacokinetics of blinatumomab. Body surface area (0.4 to 2.70 m2) influences the pharmacokinetics of blinatumomab, however, the clinical relevance of this effect is unknown.
Hepatic Impairment: No formal pharmacokinetic studies using BLINCYTO have been conducted in patients with hepatic impairment.
Renal Impairment: No formal pharmacokinetic studies of blinatumomab have been conducted in patients with renal impairment.
Pharmacokinetic analyses showed an approximately 2-fold difference in mean blinatumomab clearance values between patients with moderate renal impairment (CrCL ranging from 30 to 59 mL/min, N = 21) and normal renal function (CrCL more than 90 mL/min, N = 215). However, high interpatient variability was discerned (CV% up to 96.8%), and clearance values in renal impaired patients were essentially within the range observed in patients with normal renal function. There is no information available in patients with severe renal impairment (CrCL less than 30 mL/min) or patients on hemodialysis.
Drug Interactions: Transient elevation of cytokines may suppress CYP450 enzyme activities [see Interactions and Pharmacology: Pharmacodynamics as previously mentioned].
Specific Populations: Pediatrics: The pharmacokinetics of blinatumomab appear linear over a dose range from 5 to 30 mcg/m2/day in pediatric patients. At the recommended doses, the mean (SD) steady-state concentration (Css) values were 162 (179) and 533 (392) pg/mL at 5 and 15 mcg/m2/day doses, respectively. The estimated mean (SD) volume of distribution (Vz), clearance (CL), and terminal half-life (t1/2,z) were 3.14 (2.97) L/m2, 1.88 (1.90) L/hour/m2, and 2.04 (1.35) hours, respectively.
Toxicology: Nonclinical Toxicology: Carcinogenesis, Mutagenesis, Impairment of Fertility: No carcinogenicity or genotoxicity studies have been conducted with blinatumomab.
No studies have been conducted to evaluate the effects of blinatumomab on fertility. A murine surrogate molecule had no adverse effects on male and female reproductive organs in a 13-week repeat-dose toxicity study in mice.