Busulfan Injection administration should be supervised by a physician experienced in conditioning treatment prior to haematopoietic progenitor cell transplantation.
Busulfan Injection is administered prior to the haematopoietic progenitor cell transplantation (HCPT).
Posology: Busulfan Injection in combination with cyclophosphamide or melphalan.
In adults: The recommended dose a schedule of administration is: 0.8 mg/kg body weight (BW) of busulfan as a tow-hour infusion every 6 hours over 4 consecutive days for a total of 16 doses; followed by cyclophosphamide at 60 mg/kg/day over 2 days initiated for at least 24 hours following the 16th dose of Busulfan Injection (see Interactions).
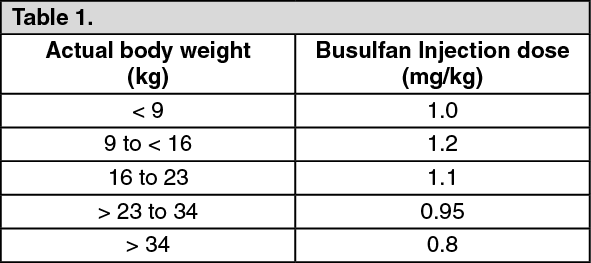
Paediatric population (0 to 17 years): The recommended dose of Busulfan Injection is as follows: See Table 1.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
followed by: 4 cycles of 50 mg/kg body weight (BW) cyclophosphamide (BuCy4) or; one administration of 140 mg/m
2 melphalan (BuMel) initiated for at least 24 hours following the 16th dose of Busulfan Injection. (See Interactions.)
Busulfan Injection is administered as a two-hour infusion every 6 hours over 4 consecutive days for a total of 16 doses prior to cyclophosphamide or melphalan and haematopoietic progenitor cell transplantation (HCPT).
Elderly patients: Patients older than 50 years of age have been successfully treated with Busulfan Injection without dose adjustment. However, for the safe use of Busulfan Injection in patients older than 60 years only limited information is available. Same dose (see Pharmacology: Pharmacokinetics under Actions) for elderly patients as for adults (<50 years old) should be used.
Busulfan Injection in combination with fludarabine (FB): In adults: The recommended dose and schedule of administration is: fludarabine administered as a single daily one-hour infusion at 30 mg/m
2 for 5 consecutive days or 40 mg/m
2 for 4 consecutive days; Busulfan Injection will be administered at 3.2 mg/kg as a single daily three-hour infusion immediately after fludarabine for 2 or 3 consecutive days.
Paediatric population (0 to 17 years): The safety and efficacy of FB in pediatric population has not been established.
Elderly patients: The administration of FB regimen has not been specifically investigated in elderly patients. However, more than 500 patients aged ≥ 55 years were reported in publications with FB conditioning regimens, yielding efficacy outcomes similar to younger patients. No dose adjustment was deemed necessary.
Obese patients: In adults: For obese patients, doing based on adjusted ideal body weight (AIBW) should be considered. Ideal body weight (IBW) is calculated as follows: IBW men (kg) = 50 + 0.91x (height in cm-152); IBW women (kg) = 45 + 0.91x (height in cm-152).
Adjusted ideal body weight (AIBW) is calculated as follows: AIBW = IBW+0.25x (actual body weight-IBW).
In paediatric population: The medicinal product is not recommended in obese children and adolescents with body mass index Weight (kg)/(m
2) >30 kg/m
2 until further data become available.
Patients with renal impairment: Studies in renally impaired patients have not been conducted, however, as busulfan is moderately excreted in the urine, dose modification is not recommended in these patients.
However, caution is recommended (see Adverse Reactions and Pharmacology: Pharmacokinetics under Action).
Patients with hepatic impairment: Busulfan Injection as well as busulfan has not been studied in patients with hepatic impairment. Caution is recommended, particularly in those patients with severe hepatic impairment (see Precautions).
Method of administration: Precautions to be taken before handling or administering the medicinal product: Busulfan Injection must be diluted prior to administration. A final concentration of approximately 0.5 mg/mL busulfan should be achieved. Busulfan Injection should be administered by intravenous infusion via central venous catheter.
For instructions on dilution of the medicinal product before administration, see Special precautions for disposal under Cautions for Usage.
Busulfan Injection should not be given by rapid intravenous, bolus or peripheral injection.
All patients should be pre-medicated with anticonvulsant medicinal products to prevent seizures reported with the use of high dose busulfan.
It is recommended to administer anticonvulsants 12 h prior to Busulfan concentrate for solution for infusion to 24 h after the last dose of Busulfan concentrate for solution for infusion.
In adult and paediatric studies, patients received either phenytoin or benzodiazepines as seizure prophylaxis treatment. (See Precautions and Interactions.)
Antiemetics should be administered prior to the first dose of Busulfan Injection and continued on a fixed schedule according to local practice through its administration.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image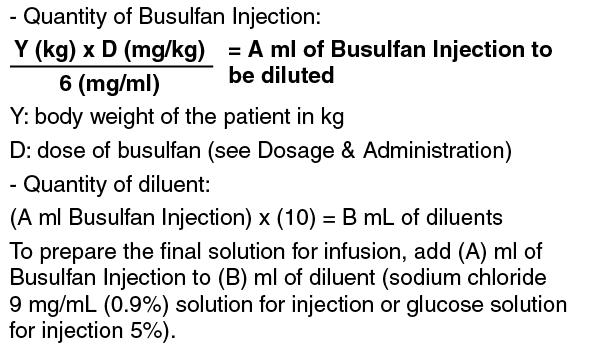 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out