Recommended General Dosing Information: The individual dosage of Cabazitaxel is based on calculation of the Body Surface Area (BSA) and is 25 mg/m
2 administered as a one-hour intravenous infusion every three weeks in combination with oral prednisone 10 mg administered daily throughout Cabazitaxel treatment.
Premedication is recommended prior to treatment.
Cabazitaxel should be administered under the supervision of a qualified physician experienced in the use of antineoplastic medicinal products. Appropriate management of complications is possible only when the adequate diagnostic and treatment facilities are readily available.
Cabazitaxel Injection single-use vial requires two dilutions prior to administration.
Do not use PVC infusion containers and polyurethane infusions sets for preparation and administration of Cabazitaxel infusion solution.
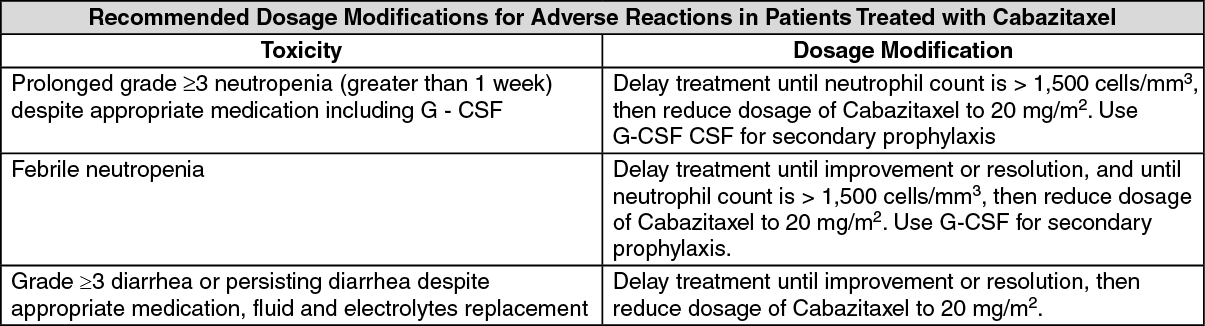
Dose modifications: The Cabazitaxel dose should be reduced to 20 mg/m if patients experience the following adverse reactions. (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Discontinue Cabazitaxel treatment if a patient continues to experience any of these reactions at 20 mg/m
2.
Premedication: Premedicate at least 30 minutes prior to each dose of Cabazitaxel with the following intravenous medications to reduce risk and/or severity of hypersensitivity:
antihistamine (dexchlorpheniramine 5 mg, or diphenhydramine 25 mg or equivalent antihistamine), corticosteroid (dexamethasone 5 mg, or diphenhydramine 25 mg or equivalent steroid), H2 antagonist (ranitidine 50 mg or equivalent H2 antagonist).
Antiemetic prophylaxis is recommended and can be given orally or intravenously as needed.
Administration Precautions: Cabazitaxel is a cytotoxic anticancer drug and caution should be exercised when handling and preparing Cabazitaxel solutions, taking into account the use of containment devices, personal protective equipment (e.g., gloves), and preparation procedures.
If Cabazitaxel Injection, diluted solutions for intravenous infusion should come into contact with the skin, immediately and thoroughly wash with soap and water. If Cabazitaxel Injection, diluted solution for intravenous infusion should come into contact with mucosa, immediately and thoroughly wash with water.
Route of Administration: Cabazitaxel Injection, 60 mg per 3 mL requires NO prior dilution with a diluent and is ready to add to the infusion solution.
Do not use PVC infusion containers or polyurethane infusions sets for preparation and administration of Cabazitaxel infusion solution.
Read this entire section carefully before diluting. Cabazitaxel requires dilutions prior to administration. Please follow the preparation instructions provided as follows.
The following dilution process must be carried out under aseptic conditions to prepare the infusion solution.
Inspect the Cabazitaxel Injection vial. The Cabazitaxel Injection is a clear colorless to pale yellow to brownish-yellow solution.
Withdraw the recommended dose from the Cabazitaxel Injection 60 mg/3 mL vial using a calibrated syringe and dilute into a sterile 250 mL PVC-free container of either 0.9% sodium chloride solution or 5% dextrose solution for infusion. If a dose greater than 65 mg of Cabazitaxel Injection is required, use a larger volume of the infusion vehicle so that a concentration of 0.26 mg/mL Cabazitaxel Injection is not exceeded.
The concentration of the Cabazitaxel Injection final infusion solution should be between 0.10 mg/mL and 0.26 mg/mL.
Cabazitaxel Injection should not be mixed with any other drugs.
Remove the syringe and thoroughly mix the final infusion solution by gently inverting the bag or bottle.
Cabazitaxel Injection final infusion solution (in either 0.9% sodium chloride solution or 5% dextrose solution) should be used within 4 hours at ambient temperature (including the one-hour infusion) or within a total of 24 hours if refrigerated (including the one-hour infusion).
As the final infusion solution is supersaturated, it may crystallize over time. Do not use if this occurs and discard.
Inspect visually for particulate matter, any crystals and discoloration prior to administration. If the Cabazitaxel Injection infusion solution is not clear or appears to have precipitation, it should be discarded.
Administration: The final Cabazitaxel infusion solution should be administered intravenously as a one-hour infusion at room temperature.
Use an in-line filter of 0.22 micrometer nominal pore size (also referred to as 0.2 micrometer) during administration.
The final Cabazitaxel infusion solution should be used immediately. However, in-use storage time can be longer under specific conditions, i.e. 8 hours under ambient conditions (including the one-hour infusion) or for a total of 24 hours if refrigerated (including the one-hour infusion).


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out