


 Sign Out
Sign Out
Capecitabine monotherapy: Safety data of capecitabine monotherapy were reported for patients who received adjuvant treatment for colon cancer and for patients who received treatment for metastatic breast cancer or metastatic colorectal cancer. The safety information includes reported data from a phase III trial in adjuvant colon cancer (995 patients treated with capecitabine and 974 treated with i.v. 5-FU/LV) and from 4 phase II trials in female patients with breast cancer (N=319) and 3 trials (1 phase II and 2 phase III trials) in male and female patients with colorectal cancer (N=630). The safety profile of capecitabine monotherapy is comparable in patients who received adjuvant treatment for colon cancer and in those who received treatment for metastatic breast cancer or metastatic colorectal cancer. The intensity of ADRs was graded according to the toxicity categories of the NCIC CTC Grading System. (See Table 4.)
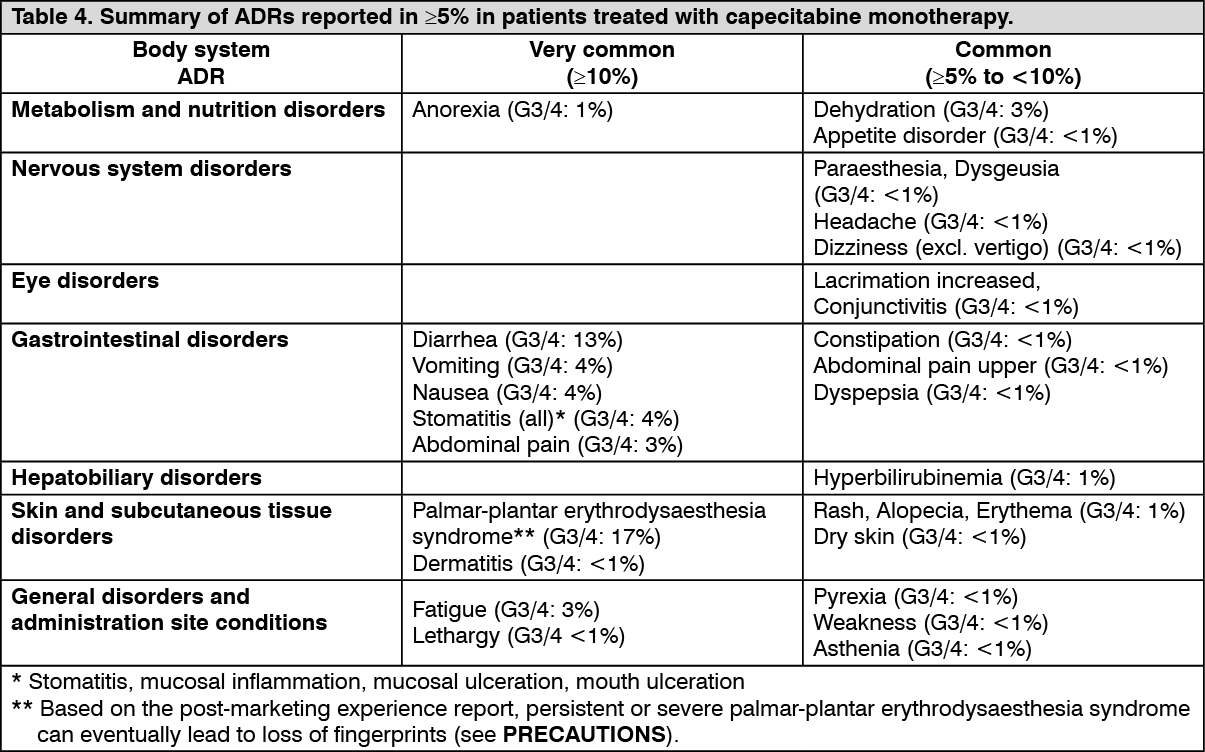 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSkin fissures were reported to be at least remotely related to Capecitabine in less than 2% of the patients in seven completed clinical trials (N=949). The following ADRs represent known toxicities with fluoropyrimidine therapy and were reported to be at least remotely related to capecitabine in less than 5% of patients in seven completed clinical trials (N=949): Gastrointestinal disorders: dry mouth, flatulence, ADRS related to inflammation/ulceration of mucous membranes such as esophagitis, gastritis, duodenitis, colitis, gastrointestinal hemorrhage.
Cardiac disorders: edema lower limb, cardiac chest pain including angina, cardiomyopathy, myocardial ischemia/infarction, cardiac failure, sudden death, tachycardia, atrial arrhythmias including atrial fibrillation, and ventricular extrasystoles.
Nervous system disorders: taste disturbance, insomnia, confusion, encephalopathy, and cerebellar signs such as ataxia, dysarthria, impaired balance, abnormal coordination.
Infections and infestations: ADRs related to bone marrow depression, immune system compromise, and/or disruption of mucous membranes, such as local and fatal systemic infections including bacterial, viral, fungal etiologies) and sepsis.
Blood and lymphatic system disorders: anemia, bone marrow depression/pancytopenia.
Skin and subcutaneous tissue disorders: pruritus, localized exfoliation, skin hyperpigmentation, nail disorders, photosensitivity reactions, radiation recall syndrome.
General disorders and administration site conditions: pain in limb, chest pain (non-cardiac).
Eye: eye irritation.
Respiratory: dyspnoea, cough.
Musculoskeletal: back pain, myalgia, arthralgia.
Psychiatric disorders: depression.
Hepatic failure and cholestatic hepatitis have been reported during clinical trials and post-marketing exposure. A causal relationship with capecitabine treatment has not been reported.
Capecitabine in combination therapy: Table 5 lists ADRs associated with the use of capecitabine in combination therapy with different chemotherapy regimens in multiple indications and occurred in addition to those seen with monotherapy and/or at a higher frequency grouping. The safety profile was similar across all indications and combination regimens. These reactions occurred in ≥5% of patients treated with capecitabine in combination with other chemotherapies. Adverse drug reactions are added to the appropriate category in the table as follows according to the highest incidence reported in any of the major clinical trials. Some of the adverse reactions are reactions commonly reported with chemotherapy (e.g. peripheral sensory neuropathy with docetaxel or oxaliplatin) or with bevacizumab (e.g. hypertension); however, an exacerbation by capecitabine therapy cannot be excluded. (See Table 5.)
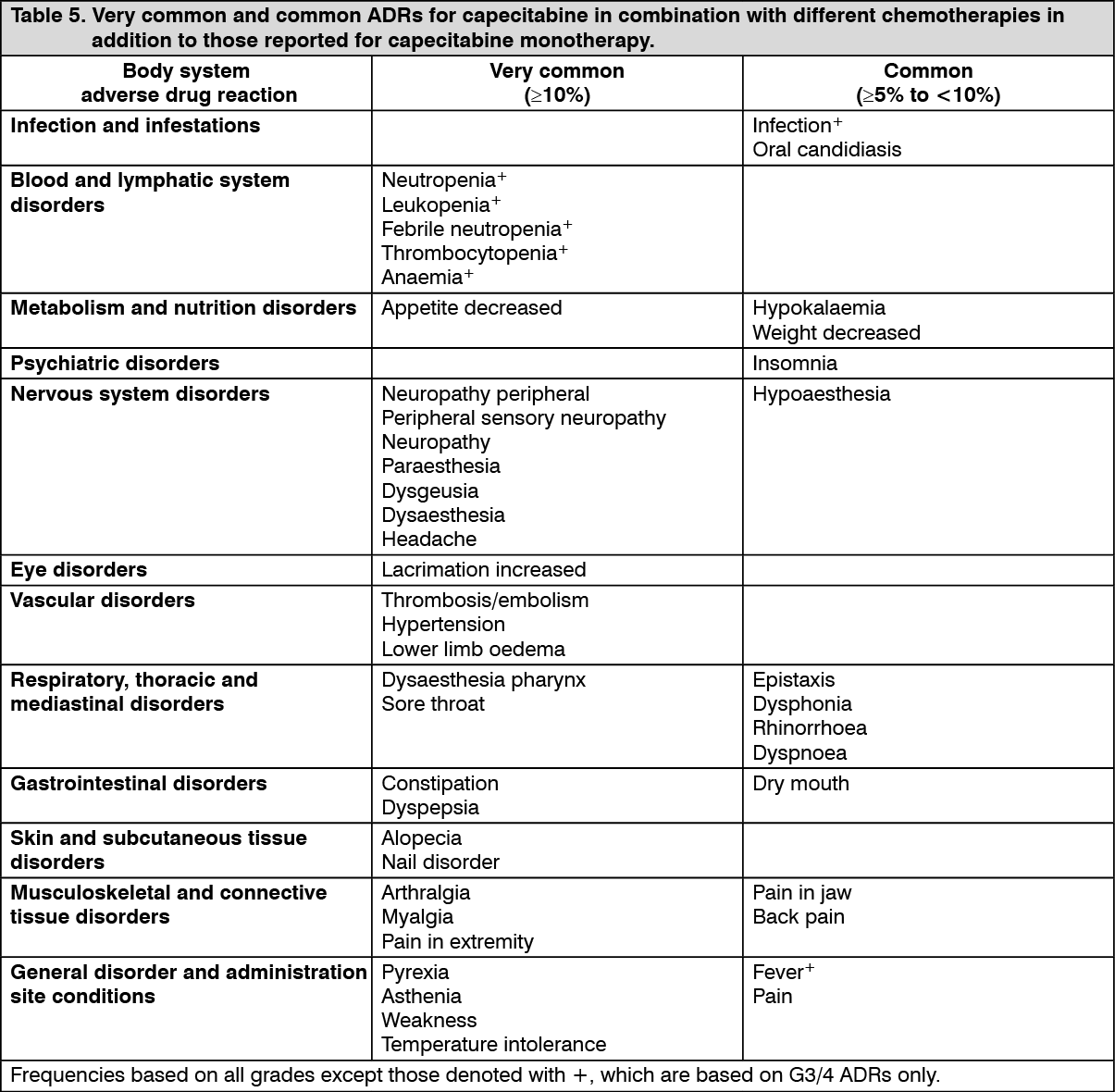 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageHypersensitivity reactions (2%) and cardiac ischaemia/infarction (3%) have been reported commonly for capecitabine in combination with other chemotherapy but in less than 5% of patients.
Rare uncommon ADRS reported for capecitabine in combination with other chemotherapy are consistent with the ADRS reported for capecitabine monotherapy or the combination product monotherapy (see prescribing information for the combination product).
Laboratory abnormalities: The following table displays laboratory abnormalities reported in 995 patients (adjuvant colon cancer) and 949 patients (metastatic breast and colorectal cancer), regardless of relationship to treatment with capecitabine. (See Table 6.)
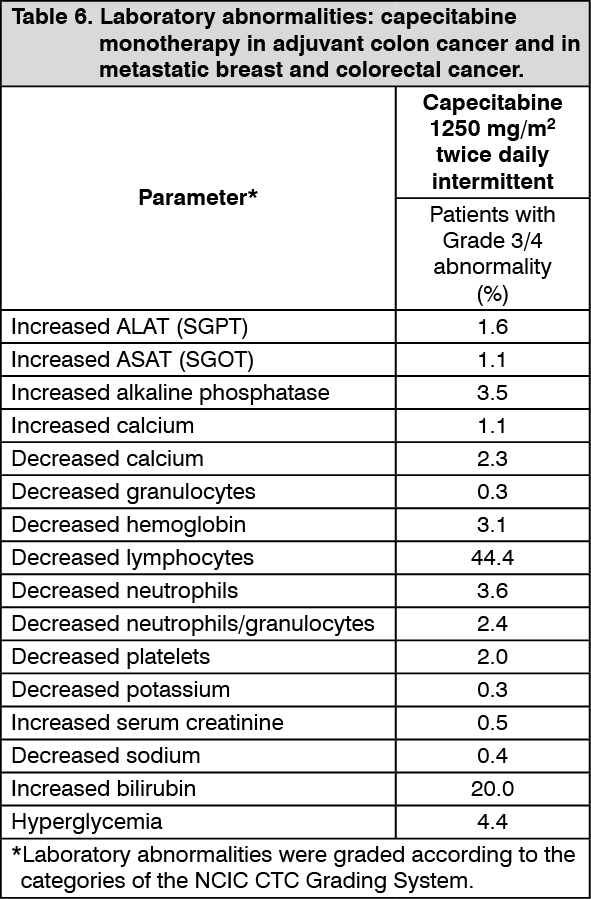 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePost-marketing experience report: The following ADRs have been reported during post-marketing experience with capecitabine based on spontaneous case reports and literature cases. Adverse drug reactions are listed according to system organ classes in MedDRA and the corresponding frequency category estimation for each adverse drug reaction is based on the following convention: very common (≥ 1/10); common (≥1/100 to <1/10); and uncommon (≥1/1,000 to <1/100); rare (≥ 1/10,000 to <1/1,000); very rare (<1/10,000); unknown (cannot be estimated from the available data). (See Table 7.)
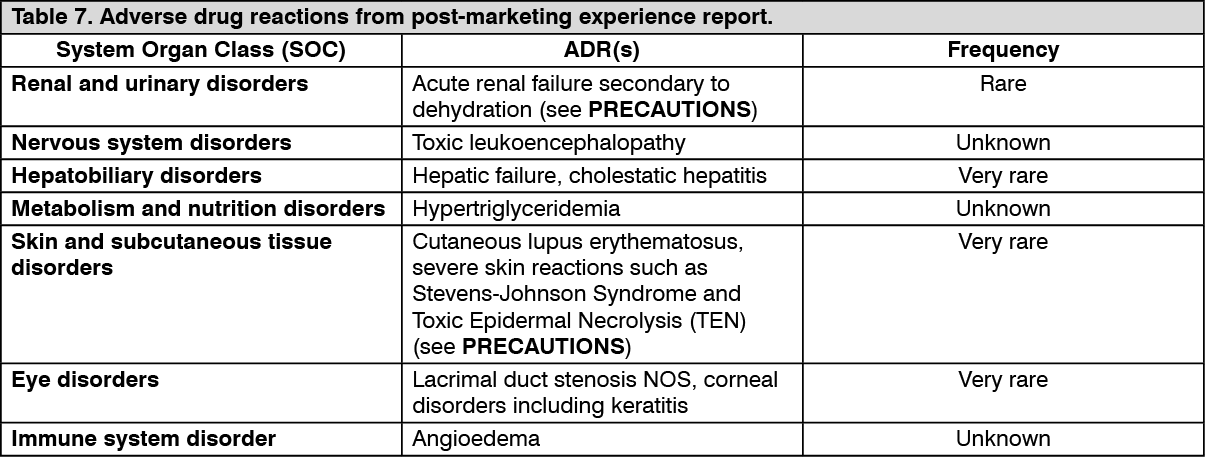 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageExposure to crushed or cut capecitabine tablets: In the instance of exposure to crushed or cut capecitabine tablets, the following ADRs have been reported: eye irritation, eye swelling, skin rash, headache, paresthesia, diarrhea, nausea, gastric irritation, and vomiting.
View ADR Monitoring Form