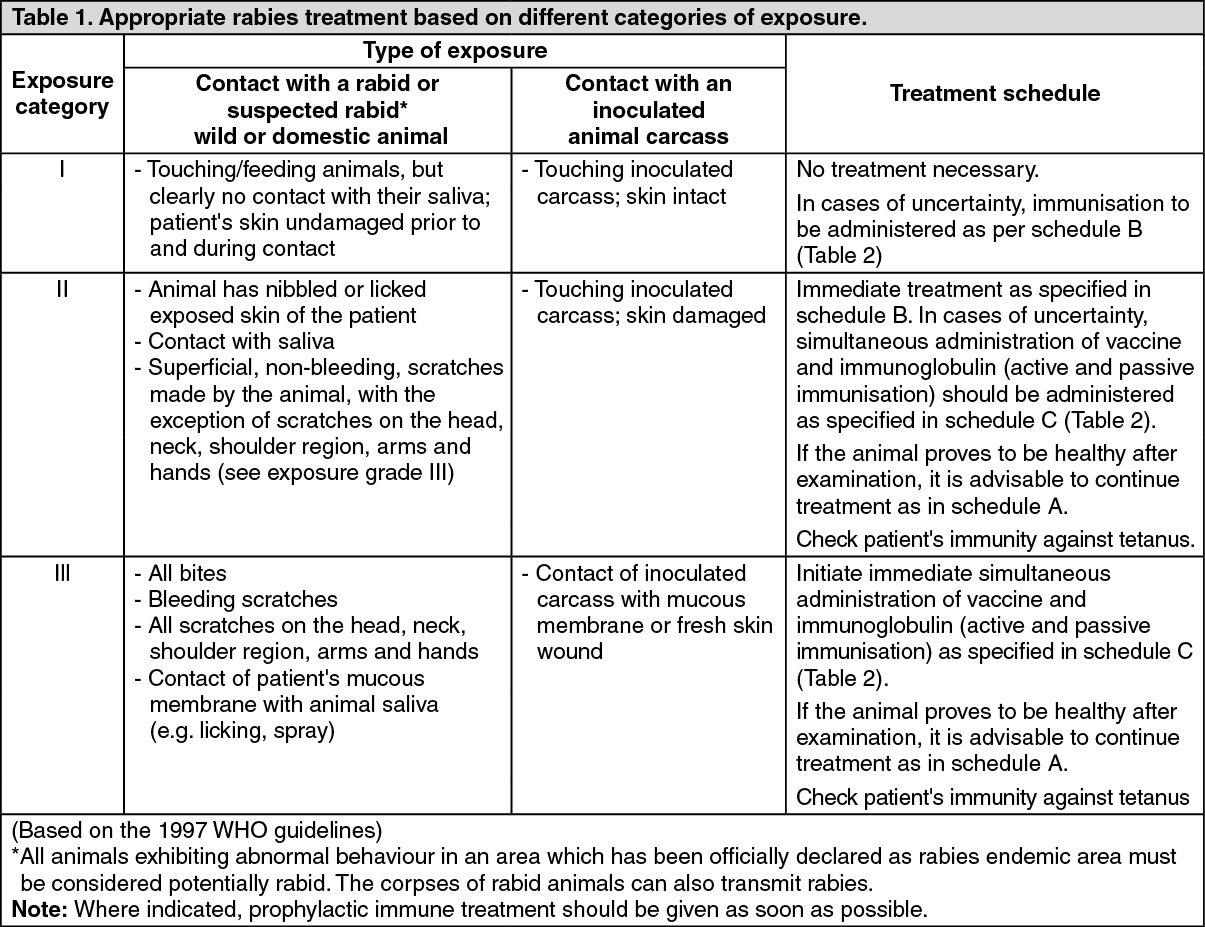
See Table 1.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
See Table 2.
Click on icon to see table/diagram/image
Additional information: This vaccine conforms to the World Health Organisation WHO requirements and contains no preservative.
The antibody concentration achieved by the immunisation falls gradually: booster doses are therefore required to maintain immunity.
All immunisations and all immunoglobulins administered should be entered by the doctor, with the name of the preparation (proprietary name) and Lot. No. in the international immunisation record.
Optimal immunity will only be conferred if the full immunisation schedule is completed.
Dosage: With ChiroRab, it is possible to vaccinate persons of any age group. The recommended single dose is 1 ml.
PRE-EXPOSURE IMMUNISATION (prior to exposure): Immunisation according to schedule A (see Table 2).
One vaccination (1 ml) on days: 0, 7 and 21 or 28.
BOOSTER DOSES: International recommendations (WHO, ACIP-US) are as follows: For persons at continuous risk, evaluate the rabies virus neutralizing antibody titres by RFFIT, every 6 months.
For persons at frequent risk, the WHO recommends antibody titre estimations every year, whereas the ACIP advocates testing every 2 years.
If titres are below 0.5 IU/ml at any time, one booster dose should be administered.
Considering the long term satisfactory antibody titres observed with ChiroRab, if serological tests cannot be conducted due to cost considerations or inaccessible medical facilities, a booster dose one year alter primary immunisation followed by one dose every 5 years would be advisable.
POST-EXPOSURE TREATMENT (after exposure): Begin with the course of immunisation immediately. For "immediate wound treatment", see "Special precaution for use"!
For indications for use, see Table 1.
1.
Unimmunised or incompletely immunised individuals (including those who have previously received fewer than 3 doses of vaccine, or who have received a vaccine of doubtful potency or origin): Treatment according to schedule B or C (see also Table 2).
One single dose of vaccine on days 0, 3, 7, 14, 28 (5-dose schedule).
As an alternative to the above mentioned 5-dose schedule, the World Health Organisation (WHO) also recommends the abbreviated 2-1-1 regimen as being effective: Two doses on day 0 (one dose given into the right and one dose into the left deltoid muscle (upper-arm muscle) or, in small children, one dose each into the anterolateral region of the right and left thigh), and one dose each on days 7 and 21 (see also Table 2. schedule B/C).
In all injuries caused by rabid animals or animals suspected to be rabid. or after contact between the saliva of these animals and the mucous membranes or damaged skin of the patient (see Table 1), the 5-dose schedule or 2-1-1 schedule along with additional passive immunisation are required (see Table 2, schedule C). 20 IU/kg bodyweight (BW) of human rabies immunoglobulin or 40 IU/kg of equine rabies immunoglobuhn are to be given once at the time of the first vaccination. As much of the rabies immunoglobulin preparation as is anatomically feasible should be applied as deeply as possible in and around the wound. Any remaining rabies immunoglobulin should be administered intramuscularly (preferably intragluteally) at a site distant from the site of the vaccine injection.
If rabies immunoglobulin is not available at the time of the first vaccination it must be administered no later than 7 days after the first vaccination since later administration would result in interference with antibody formation.
Rabies immunoglobulin should only be administered at the recommended dose.
The recommended immunoglobulin dose should neither be increased, nor decreased, nor should rabies immunoglobulin administration be repeated (for further details refer to the manufacturer's information).
The immunisation schedule must be followed exactly even if considerable time has elapsed since exposure.
In subjects at particularly high risk of contracting rabies infection (e.g. with multiple wounds particularly on the head or other markedly innervated parts of the body), or for those who have delayed initiation of treatment, the patient must be vaccinated on each of the days 0, 3, 7, 14, 28. Additionally the initial immunisation dose should be doubled: a single dose of vaccine should be given by injection soon as possible after exposure into the right deltoid and another single dose into the left deltoid muscle, or in small children, a single dose given in to the anterolateral region of the right thigh with another single dose given into the left thigh.
2. Previously fully immunised individuals: Patients who have previously received a complete course of primary immunisation (pre- or post-exposure) should receive two doses of ChiroRab; one on each of days 0 and 3, respectively. This is independent of the interval to the last immunisation. No administration of rabies immunoglobulin is required.
3. lmmunocompromised individuals: Patients receiving immunosuppressive therapy or who have congenital or acquired immunodeficiency, should be vaccinated once on each of the days 0, 3, 7, 14 28. In addition, the initial immunisation dose (day 0) should be doubled with a single dose of vaccine being administered as soon as possible after exposure into each of the right and left deltoid muscles (upper-arm muscle) or, in small children, into the anterolateral region of each of the right and left thighs.
If immunocompromised patients (with impaired defence system) are treated after exposure to rabies, it is advisable that the antibody titre be measured 14 days after the first dose. If a titre of at least 0.5 IU/ml, which is considered adequate to confer protection, is not present, a dose of vaccine should be immediately administered into each upper-arm (or into each thigh IN the case of small children). Depending on the immunisation status of these patients, additional doses may be necessary to achieve appropriate antibody titres in serum (for information on immunoglobulin administration see Unimmunised or incompletely immunised individuals in the previous text).
Method and duration of administration: The lyophihsate should be reconstituted immediately using the diluent supplied, and carefully agitated prior to injection. The reconstituted vaccine should be used immediately.
ChiroRab must be given by intramuscular injection into the deltoid muscle (upper-arm muscle), or into the anterolateral region of the thigh in small children. The vaccine must not be given by intragluteal (in the gluteal muscle injection).
The vaccine must not be administered by intravascular (in a blood vessel) injection.
Intradermal schedule: The WHO recognises the effectiveness of modern issue culture rabies vaccines when given by the intradermal route (i.d.) for post exposure immunisation. The WHO recommends the use of 0.1 ml ChiroRab for intradermal use for the Thai Red Cross (TRC) 2-2-2-0-1-1 regimen. The intradermal use of 0.1 ml ChiroRab has been proven to be well-tolerated, immunogenic and efficacious. Furthermore, the WHO has recently updated the recommendations for the TRC regimen to be used also in a 2-2-2-0-2 schedule. If ChiroRab is to be administered by the intradermal route, the following instructions and warnings must be strictly adhered to:
Dosage and administration (post-exposure): One i.d. dose comprised of 0.1 ml of the total reconstituted vaccine, is to be administered tn the upper arm, over the deltoid.
Non-vaccinated individuals: The 2-site intradermal method (2-2-2-0-1-1) also known as the TRC schedule is recommended: one i.d. injection of 0.1 ml over each left and right deltoid on days 0, 3, 7.
One i.d. injection of 0.1 ml at a single site on upper arm (deltoid) on day 28 (or 30) and day 90. (Alternatively, the i.d. injection for day 90 can be administered as a second dose on day 28 (or 30)). This schedule is the updated TAC regimen (2-2-2-0-2).
Fully vaccinated individuals: (see above definition): Immediate booster injection of a single dose of 0.1 ml on days 0, 3.
Special precautions for the intradermal route: It is essential hat intradermal administration of vaccine be administered only by medical staff trained in the i.d. technique in order to ensure that the vaccine is delivered intradermally and not subcutaneously. For the intradermal route a sterile syringe with fixed needle (insulin type) is preferred. A separate sterile needle and syringe must be used for each patient. Correct intradermal injection should result in a raised papule with an orange peel appearance. If the vaccine has been injected too deeply and a papule is not observed, the needle should be withdrawn and vaccine re-administered nearby. WHO reoommendations for the use of rabies immunoglobulin after exposure to rabies virus should be carefully followed.
This vaccine does not contain a preservative, therefore, great care must be taken to avoid contamination of the reconstituted vaccine.
Any reconstituted vaccine should be used as soon as possible. It must be stored in a refrigerator at +2 to +8°C and used within 6 to 8 hours of reconstitution if not maintained at +2 to +8°c. The vaccine must be immediately discarded.
The i.d. route must not be used in the following instances: individuals receiving long-term corticosteroid or other immunosuppressive therapy or chloroquine; immunocompromised individuals.
This vaccine is of sufficient potency to allow its safe use in one of the WHO recommended intradermal post-exposure regimens in countries where relevant national authorities have approved the use of the intradermal route for rabies post-exposure prophylaxis.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image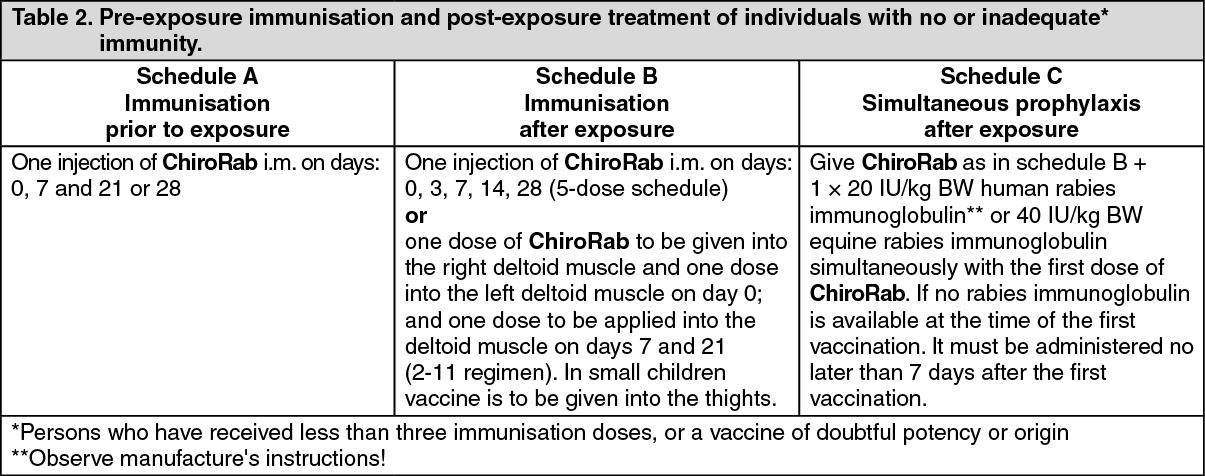 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out