CLINOLEIC 20% contains 200 mg/ml of lipids.
Route of administration: Intravenous infusion: when administered as part of a complete nutrition admixture (with glucose and amino acids) the central or peripheral venous route should be chosen depending on the osmolality of the final admixture.
In rare cases, when Infused alone as a complementary support to oral or enteral nutrition, CLINOLEIC 20% can be administered via peripheral vein.
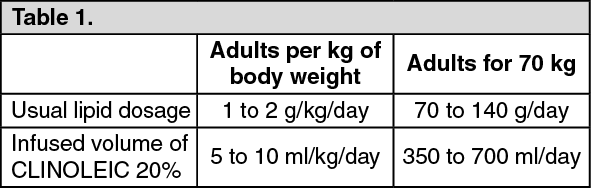
Dosage: IN ADULTS: The dosage is 1 g/kg/day to a maximum of 2 g lipids/kg/day. The initial infusion rate must be slow and not exceed 0.1 g lipids or 0.5 ml (10 drops) per minute for 10 minutes then gradually increased until reaching the required rate after half an hour. Never exceed 0.15 g lipids/kg/hour (0.75 ml/kg/hour). (See Table 1.)
 Click on icon to see table/diagram/image
IN CHILDREN:
Click on icon to see table/diagram/image
IN CHILDREN: CLINOLEIC 20% should be administered as a continuous 24h/day infusion. It is recommended not to exceed a daily dose of 3g-lipids/kg b.w. (body weight) and an infusion rate of 0.15 g lipids/kg b.w./h.
Daily dose should be increased gradually during the first week of administration.
IN PREMATURE NEWBORNS AND LOW BIRTH WEIGHT INFANTS: The use of CLINOLEIC 20% is restricted to premature infants of 28 weeks of gestational age or more.
CLINOLEIC 20% should be administered as a continuous 24h/day infusion.
The initial daily dose should be 0.5-1.0g lipids/kg b.w. The dose may be increased by 0.5-1.0g lipids/kg b.w. every 24 hours up to a daily dose of 2.0 g lipids/kg b.w.
Usage in nutritive admixtures (with glucose and amino acids): Before administration to the patient, the compatibility of the components and stability of the admixture must be checked.
Admixing should be accompanied by gentle agitation during preparation under strict aseptic conditions.
"Breaking" or "oiling out" of the emulsion can be visibly identified by accumulation of yellowish droplets or particles in the admixture.
For intravenous infusion: When used in neonates and children below 2 years, the solution (in bags and administration sets) should be protected from light exposure after admixture through administration (Precautions and Instructions for Use/Handling and Disposal under Cautions for Usage).
It is recommended that after opening the bag, the contents should be used immediately, and should not be stored for a subsequent infusion.
The dosage depends on energy expenditure, the patient's clinical status, body weight, and ability to metabolize CLINOLEIC 20%, as well as additional energy given orally/enterally. Therefore, the dosage should be individualized and the bag size chosen accordingly.
The maximum daily dose of CLINOLEIC 20% should be based on individual total nutritional requirements and patient tolerance.
CLINOLEIC 20% can be administered via the central or peripheral route when infused alone as a complementary support to oral or enteral nutrition. When administered as an admixture (e.g., together with dextrose and/or amino acids) the route of administration should be chosen based on the final osmolarity of the infusate.
The administration flow rate must be adjusted taking into account the dose being administered, the daily volume intake, and the duration of the infusion (see OVERDOSAGE).
The recommended duration of infusion for a parenteral nutrition bag is between 12 and 24 hours, depending on the clinical situation. Treatment with parenteral nutrition may be continued for as long as is required by the patient's condition.
Use of a final filter is recommended during administration of all parenteral nutrition solutions, where possible.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
