Summary of the safety profile: The most common adverse reactions are phlebitis, pseudo-allergic reactions and flushing of the upper body ("red-neck syndrome") in connection with too rapid intravenous infusion of vancomycin.
List of adverse reactions: Within each frequency grouping, undesirable effects are presented in order of decreasing seriousness.
The adverse reactions listed as follows are defined using the following MedDRA: Very common (≥1/10); Common (≥1/100 to <1/10); Uncommon (≥1/1,000 to <1/100); Rare (≥1/10,000 to <1/1,000); Very rare (<1/10,000); Not known (cannot be estimated from the available data).
Blood and the lymphatic system disorder: Rare: Reversible neutropenia, agranulocytosis, eosinophilia, thrombocytopenia, pancytopenia.
Immune system disorders: Rare: Hypersensitivity reactions, anaphylactic reactions.
Ear and labyrinth disorders: Uncommon: Transient or permanent loss of hearing.
Rare: Vertigo, tinnitus, dizziness.
Cardiac disorders: Very rare: Cardiac arrest.
Vascular disorders: Common: Decrease in blood pressure.
Rare: Vasculitis.
Respiratory, thoracic and mediastinal disorders: Common: Dyspnoea, stridor.
Gastrointestinal disorders: Rare: Nausea.
Very rare: Pseudomembranous enterocolitis.
Not known: Vomiting, diarrhoea.
Skin and subcutaneous tissue disorders: Common: Flushing of the upper body ("red man syndrome"), exanthema and mucosal inflammation, pruritus, urticaria.
Very rare: Exfoliative dermatitis, Stevens-Johnson syndrome, Lyell's syndrome, Linear IgA bullous dermatosis.
Not known: Eosinophilia and systemic symptoms (DRESS syndrome), AGEP (acute generalised exanthematous pustulosis).
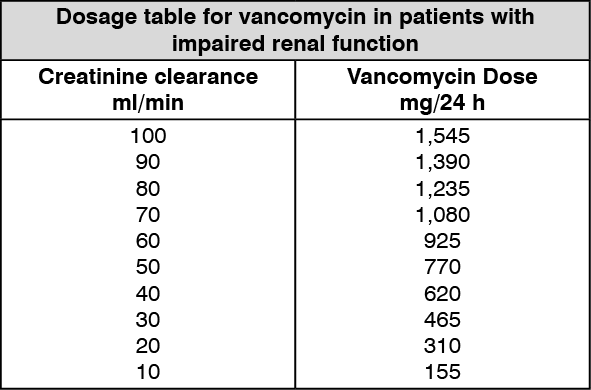
Renal and urinary disorders: Common: Renal insufficiency manifested primarily by increased serum creatinine and serum urea.
Rare: Interstitial nephritis, acute renal failure.
Not known: Acute tubular necrosis.
General disorders and administration site conditions: Common: Phlebitis, redness of the upper body and face.
Rare: Drug fever, shivering, pain and muscle spasm of the chest and back muscles.
Description of selected adverse drug reactions: Reversible neutropenia usually starting one week or more after onset of intravenous therapy or after total dose of more than 25 g.
Intravenous vancomycin should be infused slowly. During or shortly after rapid infusion anaphylactic/anaphylactoid reactions including wheezing may occur.
The reactions abate when administration is stopped, generally between 20 minutes and 2 hours. Vancomycin should be infused slowly (see Dosage & Administration and Precautions). Necrosis may occur after intramuscular injection.
Tinnitus, possibly preceding onset of deafness, should be regarded as an indication to discontinue treatment.
Ototoxicity has primarily been reported in patients given high doses, or in those on concomitant treatment with other ototoxic medicinal product like aminoglycoside, or in those who had a pre-existing reduction in kidney function or hearing.
If a bullous disorder is suspected, the medicinal product should be discontinued and specialised dermatological assessment should be carried out.
Paediatric population: The safety profile is generally consistent among children and adult patients. Nephrotoxicity has been described in children, usually in association with other nephrotoxic agents such as aminoglycosides.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
