PHARMACOLOGY: Mechanism of Action: Influenza illness and its complications may follow influenza infection. Global surveillance of influenza viruses identifies yearly antigenic variants. Since 1977, antigenic variants of influenza A (H1N1 and H3N2) viruses and influenza B viruses have been in global circulation. Specific levels of hemagglutination inhibition (HI) antibody titer post-vaccination with inactivated influenza virus vaccines have not been correlated with protection from influenza virus infection. In some human studies, antibody titers ≥1:40 have been associated with protection from influenza illness in up to 50% of participants.
Antibodies against one influenza virus type or subtype confer limited or no protection against another. Furthermore, antibodies to one antigenic variant of influenza virus might not protect against a new antigenic variant of the same type or subtype. Frequent development of antigenic variants through antigenic drift is the virologic basis for seasonal epidemics and the reason for the usual change of one or more new strains in each year's influenza vaccine. Therefore, influenza vaccines are standardized to contain the hemagglutinins of influenza virus strains representing the influenza viruses likely to be circulating in the U.S. during the influenza season.
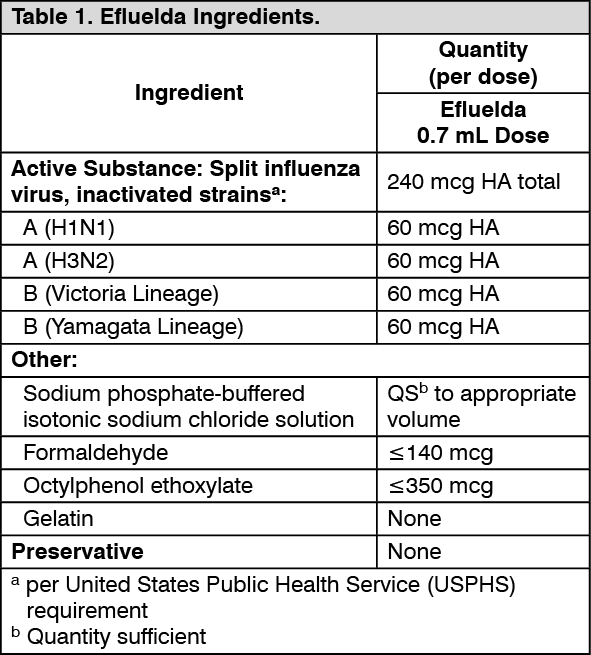
Efluelda stimulates the immune system to produce antibodies that help prevent influenza disease.
NONCLINICAL TOXICOLOGY: Carcinogenesis, Mutagenesis, Impairment of Fertility: Efluelda has not been evaluated for carcinogenic or mutagenic potential or for impairment of fertility.
CLINICAL STUDIES: Immunogenicity of Efluelda in Adults 65 Years of Age and Older: Study 1 (NCT03282240, see http://clinicaltrials.gov) was a randomized, active-controlled, modified double-blind trial in adults 65 years of age and older conducted in the US. The study compared the safety and immunogenicity of Efluelda to those of Fluzone High-Dose. The objective was to demonstrate immunologic non-inferiority of Efluelda to Fluzone High-Dose, as assessed by HAI geometric mean antibody titers (GMTs) at Day 28 and seroconversion rates, to strains common to formulations of both vaccines, based on pre-specified criteria.
A total of 2670 adults from 65 years of age were randomized (4:1:1) to receive one dose of either Efluelda or one of two formulations of Fluzone High-Dose (one formulation contained a B strain of the Victoria lineage [TIV-HD1] while the other contained a B strain of the Yamagata lineage [TIV-HD2]).
Females accounted for 58.2% of participants in the Efluelda group and 57.4% of participants in the Fluzone High-Dose group (TIV-HD1 and TIV-HD2, pooled). The mean age was 72.9 years (range: 65 through 100 years) in the Efluelda group and the mean age was 73.0 (range: 65 through 95 years) in the Fluzone High-Dose group. The percentage of subjects 75 years of age or older was 35.4% in the Efluelda group and 35.8% in the Fluzone High-Dose group. Most participants were White (91.2% and 89.7%), followed by Black (6.8% and 8.0%), and Hispanic (2.8% and 2.6%) in the Efluelda and Fluzone High-Dose groups, respectively.
The immunogenicity results of Study 1 are summarized in Table 2 and Table 3 as follows. (See Tables 2 and 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Efluelda was as immunogenic as Fluzone High-Dose for GMTs and seroconversion rates for the common influenza strains. Efluelda induced a superior immune response, based on a pre-specified superiority criterion, with respect to the additional B strain than the immune response induced by Fluzone High-Dose formulation that did not contain the additional B strain.
Efficacy of Fluzone High-Dose in Adults 65 Years of Age and Older: The efficacy of Fluzone High-Dose (trivalent formulation) is relevant to Efluelda since both vaccines are manufactured according to the same process and have overlapping compositions.
Study 2 (NCT01427309) was a multi-center, double-blind, post-licensure efficacy trial conducted in the U.S. and Canada in which adults 65 years of age and older were randomized (1:1) to receive either Fluzone High-Dose or Fluzone. The study was conducted over two influenza seasons (2011-2012 and 2012-2013); 53% of participants enrolled in the first year of the study were re-enrolled and re-randomized in the second year. The per-protocol analysis set for efficacy assessments included 15,892 Fluzone High-Dose recipients and 15,911 Fluzone recipients. The majority (67%) of participants in the per-protocol analysis set for efficacy had one or more high-risk chronic comorbid conditions.
In the per-protocol analysis set, females accounted for 57.2% of participants in the Fluzone High-Dose group and 56.1% of participants in the Fluzone group. In both groups, the median age was 72.2 years (range 65 through 100 years). Overall, most participants in the study were White (95%); approximately 4% of study participants were Black, and approximately 6% reported Hispanic ethnicity.
The primary endpoint of the study was the occurrence of laboratory-confirmed influenza (as determined by culture or polymerase chain reaction) caused by any influenza viral type/subtype in association with influenza-like illness (ILI), defined as the occurrence of at least one of the following respiratory symptoms: sore throat, cough, sputum production, wheezing, or difficulty breathing; concurrent with at least one of the following systemic signs or symptoms: temperature >99.0°F (>37.2°C), chills, tiredness, headaches or myalgia. Participants were monitored for the occurrence of a respiratory illness by both active and passive surveillance, starting 2 weeks post-vaccination for approximately 7 months. After an episode of respiratory illness, nasopharyngeal swab samples were collected for analysis; attack rates and vaccine efficacy were calculated (see Table 4).
Click on icon to see table/diagram/image
A secondary endpoint of the study was the occurrence of culture-confirmed influenza caused by viral types/subtypes antigenically similar to those contained in the respective annual vaccine formulations in association with a modified CDC-defined ILI, defined as the occurrence of a temperature >99.0°F (>37.2°C) with cough or sore throat. The efficacy of Fluzone High-Dose relative to Fluzone for this endpoint was 51.1% (95% CI: 16.8; 72.0).
Effectiveness of TIV-HD in Adults 65 Years of Age and Older: Randomised Clinical Trials: A cluster-randomised, controlled clinical trial in United States nursing homes assessed the relative effect of TIV-HD versus a standard dose of influenza vaccine in hospitalisations among 53,008 individuals during the 2013-2014 influenza season.
During the 2013-2014 season, when adjusting for the pre-specified patient and facility characteristics, the incidence of respiratory-related hospital admissions (primary objective) was significantly reduced in facilities where residents received TIV-HD compared with those that received standard-dose influenza vaccines by 12.7% (adjusted risk ratio [ARR] 0.873, 95% CI 0.776 to 0.982, p=0.023). Moreover, with respect to secondary endpoints, TIV-HD reduced hospital admissions for pneumonia by 20.9% (ARR 0.791, 95% CI: 0.267 to 0.953, p=0.013) and all-cause hospital admissions by 8% (ARR 0.915, 95% CI: 0.863 to 0.970, p=0.0028).
Observational Studies: Several retrospective studies, over 10 influenza seasons and in more than 34 million individuals 65 years of age and older, confirmed the superior protection offered by TIV-HD compared to standard-dose influenza vaccines against complications of influenza such as pneumonia hospitalisation (27.3% [95% CI 15.3-37.6%], p<0.001), cardio-respiratory hospitalisations (17.9% [95% CI 15.0-20.8%], p<0.001) and all-cause hospitalisation (8.4% [95% CI 5.7-11.0%], p<0.001); although the impact may vary per season.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image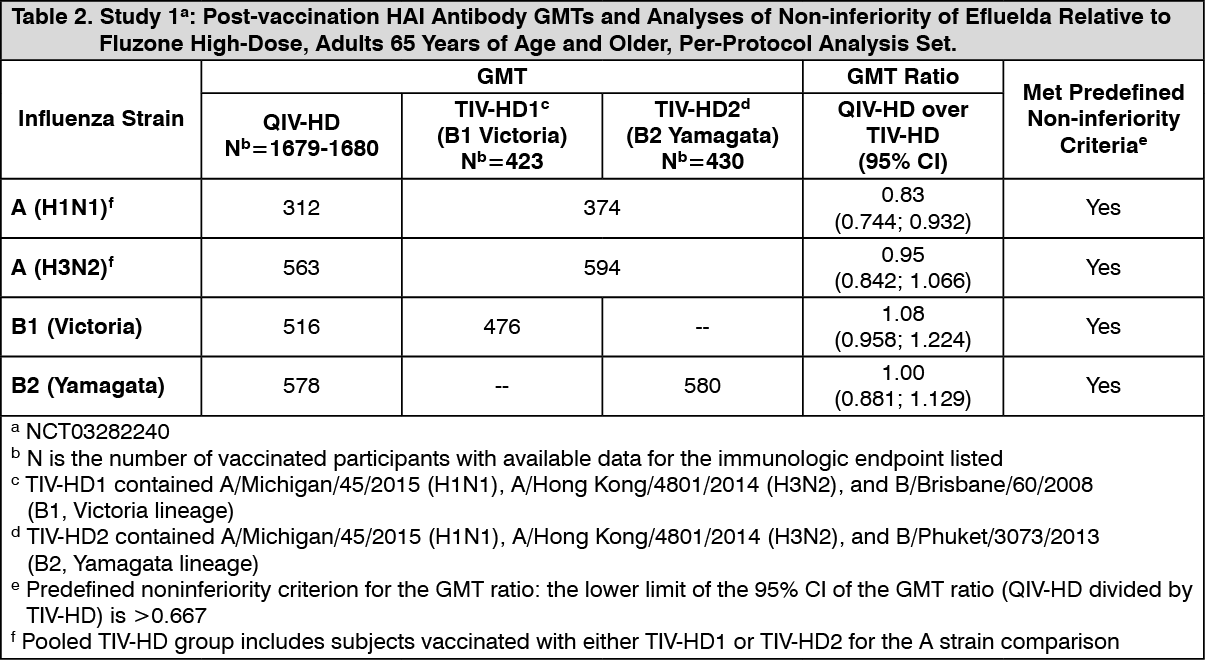 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image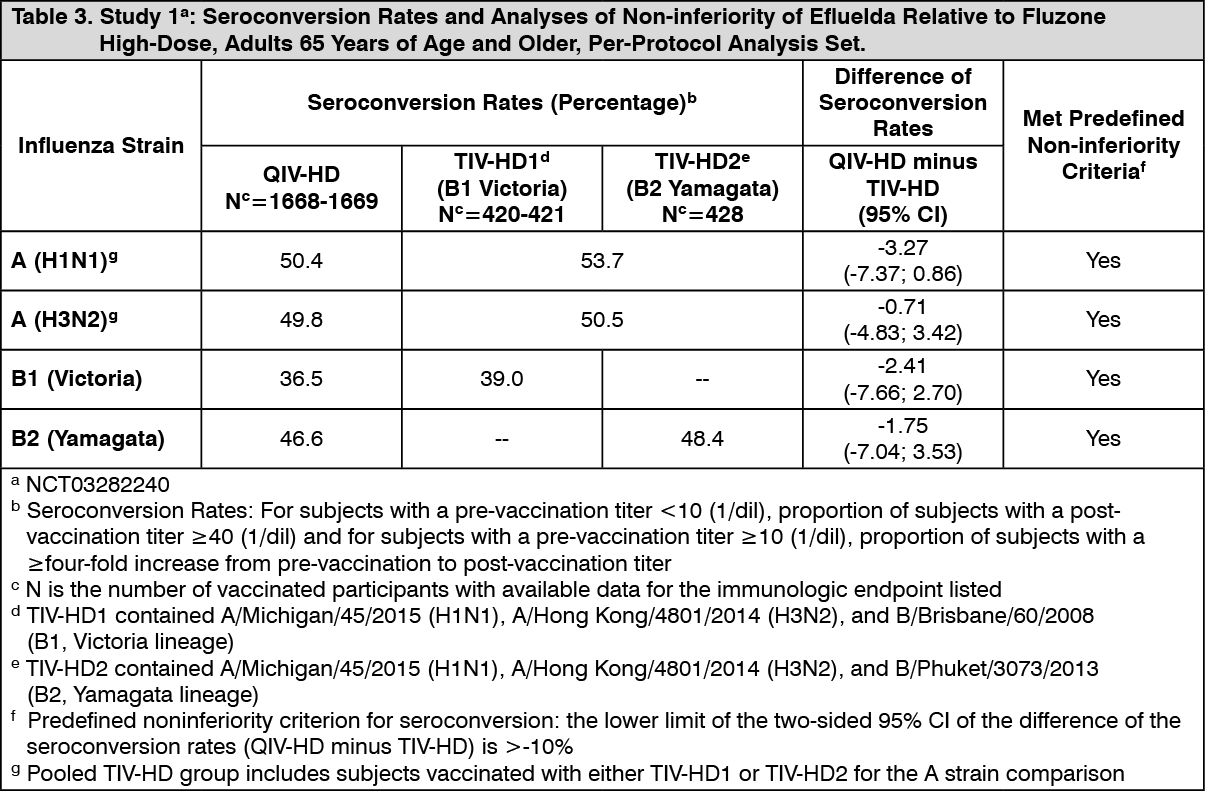 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image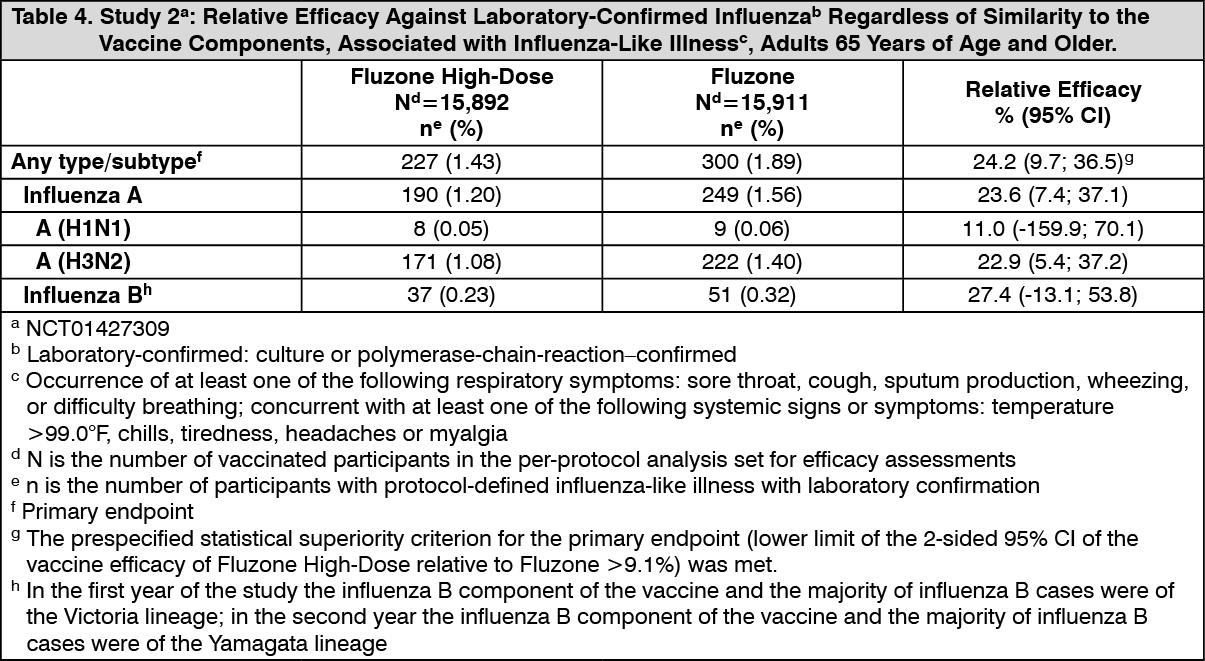 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
