


 Sign Out
Sign Out

Anidulafungin selectively inhibits 1,3-β-D glucan synthase, an enzyme present in fungal, but not mammalian cells. This results in inhibition of the formation of 1,3-β-D-glucan, an essential component of the fungal cell wall. Anidulafungin has shown fungicidal activity against Candida species and activity against regions of active cell growth of the hyphae of Aspergillus fumigatus.
Activity in vitro: Anidulafungin is active in vitro against Candida spp. including C. albicans, C. glabrata, C. krusei, C. parapsilosis, C. tropicalis, C. dubliniensis, C. lusitaniae, and C. guilliermondii and Aspergillus species including A. fumigatus, A. flavus, A. niger, and A. terreus. Its activity is not affected by resistance to other classes of antifungal agents.
MICs were determined according to the Clinical and Laboratory Standard Institute (CLSI) approved standard reference methods M27 and M38. The relationship between clinical response and in vitro activity remains to be elucidated.
There have been reports of Candida isolates with reduced susceptibility to echinocandins including anidulafungin, but the clinical significance of this observation is unknown.
Activity in vivo: Parenterally administered anidulafungin was effective against Candida spp. in immunocompetent and immunocompromised mouse and rabbit models. Anidulafungin treatment prolonged survival and also reduced the organ burden of Candida spp.
Experimental infections included disseminated C. albicans infection in neutropenic rabbits, esophageal/oropharyngeal infection of neutropenic rabbits with fluconazole-resistant C. albicans and disseminated infection of neutropenic mice with fluconazole-resistant C. glabrata.
Anidulafungin has also demonstrated activity against Aspergillus fumigatus in mouse and rabbit infection models.
In combination with other antifungal agents: In vitro studies of anidulafungin in combination with fluconazole, itraconazole and amphotericin B suggest no antagonism of antifungal activity against Candida species. The clinical significance of these results is unknown. In vitro studies have evaluated the activity of anidulafungin in combination with itraconazole, voriconazole, and amphotericin B against Aspergillus spp. The combination of anidulafungin and amphotericin B showed indifference for 16 of 26 isolates, while anidulafungin in combination with either itraconazole or voriconazole showed synergy against 18 of 26 isolates. The clinical significance of these results is unknown.
Information from Clinical Studies: Candidemia and Other Forms of Invasive Candidiasis: The safety and efficacy of anidulafungin were evaluated in a pivotal, Phase 3, randomized, double-blind, multicenter, multinational study of patients with candidemia and/or other forms of invasive candidiasis, associated with clinical signs of infection. Patients were randomized to receive once daily intravenous anidulafungin (200 mg loading dose followed by 100 mg maintenance dose) or intravenous fluconazole (800 mg loading dose followed by 400 mg maintenance dose). Patients were stratified by APACHE II score (≤20 and >20) and the presence or absence of neutropenia. Patients with Candida endocarditis, osteomyelitis or meningitis, or those with infection due to C. krusei, were excluded from the study. Treatment was administered for at least 14 and not more than 42 days. Patients in both study arms were permitted to switch to oral fluconazole after at least 10 days of intravenous therapy, provided that they were able to tolerate oral medication, were afebrile for at least 24 hours, and the most recent blood cultures were negative for Candida species.
Patients who received at least one dose of study medication and who had a positive culture for Candida species from a normally sterile site before entry into the study (modified intent-to-treat [MITT] population) were included in the primary analysis of global response at the end of intravenous therapy. A successful global response required clinical improvement and microbiological eradication. Patients were followed for six weeks beyond the end of all therapy.
Two hundred and fifty-six patients (aged 16 to 91 years) were randomized to treatment and received at least one dose of study medication. Two hundred and forty-five patients (127 anidulafungin, 118 fluconazole) met the criteria for inclusion in the MITT population. Of these, 219 patients (116 anidulafungin (91.3%), 103 fluconazole (87.3%)) had candidemia only; 5.5% patients in the anidulafungin arm and 9.3% patients in the fluconazole arm had infections at other normally sterile sites; finally 3.1% patients in the anidulafungin arm and 3.4% patients in the fluconazole arm had both (candidemia and infections at other normally sterile sites). The most frequent species isolated at baseline were C. albicans (63.8% anidulafungin, 59.3% fluconazole), followed by C. glabrata (15.7%, 25.4%), C. parapsilosis (10.2%, 13.6%) and C. tropicalis (11.8%, 9.3%). The majority (97%) of patients were non-neutropenic (ANC > 500) and 81% had APACHE II scores less than or equal to 20.
At the end of intravenous therapy, anidulafungin was superior to fluconazole in the treatment of patients with candidemia and/or other forms of invasive candidiasis. In the anidulafungin arm, 96 patients (75.6%) had global success versus 71 patients (60.2%) in the fluconazole arm. The between group difference in global success rate (anidulafungin global success rate minus fluconazole global success rate) was 15.4% (95% CI: 3.9, 27.0).
Esophageal Candidiasis: Anidulafungin was evaluated in a double-blind, double-dummy, randomized Phase 3 study. Patients were randomized to receive anidulafungin, once daily intravenous (100 mg loading dose followed by 50 mg/day) or oral fluconazole (200 mg loading dose followed by 100 mg/day). Treatment duration was 7 days beyond resolution of symptoms for a minimum of 14 and a maximum of 21 days. Of the 442 patients with culture confirmed esophageal candidiasis, 91% had C. albicans isolated at the baseline. Treatment groups were similar in demographic and other baseline characteristics. In this study, of 280 patients tested, 237 (84.6%) tested HIV positive. In both groups, the median time to resolution of symptoms was 5 days and the median duration of therapy was 14 days.
The primary endpoint was endoscopic outcome at end of therapy (EOT). Patients were considered clinically evaluable if they received at least 10 days of therapy, had an EOT assessment with a clinical outcome other than 'indeterminate', had an endoscopy at EOT, and did not have any protocol violations prior to the EOT visit that would affect an assessment of efficacy. An endoscopic success, defined as cure (endoscopic grade of 0 on a 4 point severity scale) or improvement (decrease of one or more grades from baseline), was seen in 225/231 (97.4%) anidulafungin-treated patients and 233/236 (98.7%) fluconazole-treated patients. The majority of these patients were endoscopic cures (grade=0). The between group difference in global success rate (anidulafungin minus fluconazole) was -1.3% (95% CI: -3.8, 1.2).
Two weeks after completing therapy, the anidulafungin group had significantly more endoscopically-documented relapses than the fluconazole group, 120/225 (53.3%) vs. 45/233 (19.3%), respectively. The between group treatment difference (anidulafungin minus fluconazole) was 34% (95% CI: 25.8, 42.3).
Clinical success (cure or improvement in clinical symptoms including odynophagia/dysphagia and retrosternal pain) occurred in 229/231 (99.1%) of the anidulafungin-treated patients and 235/236 (99.6%) of the fluconazole-treated patients at the end of therapy. For patients with C. albicans, microbiological success occurred in 142/162 (87.7%) of the anidulafungin-treated group and 157/166 (94.6%) of the fluconazole-treated group at the end of therapy. For patients with Candida species other than C. albicans, success occurred in 10/12 (83.3%) of the anidulafungin-treated group and 14/16 (87.5%) of the fluconazole-treated group.
Candida Infections in Neutropenic Patients: The efficacy of anidulafungin (200 mg intravenous loading dose followed by 100 mg intravenous daily) in adult neutropenic patients (defined as absolute neutrophil count ≤500 cells/mm3, WBC ≤500 cells/mm3 or classified by the investigator as neutropenic at baseline) with microbiologically confirmed invasive candidiasis was assessed in an analysis of pooled data from 5 prospective studies (1 comparative versus caspofungin and 4 open-label, non-comparative). Patients were treated for at least 14 days. In clinically stable patients, a switch to oral azole therapy was permitted after at least 5 to 10 days of treatment with anidulafungin. A total of 46 patients were included in the analysis. The majority of patients had candidemia only (84.8%; 39/46). The most common pathogens isolated at baseline were C. tropicalis (34.8%; 16/46), C. krusei (19.6%; 9/46), C. parapsilosis (17.4%; 8/46), C. albicans (15.2%; 7/46), and C. glabrata (15.2%; 7/46). The successful global response rate at End of Intravenous Treatment (primary endpoint) was 26/46 (56.5%) and End of All Treatment was 24/46 (52.2%). All-cause mortality up to the end of the study (6 Week Follow-up Visit) was 21/46 (45.7%).
The efficacy of anidulafungin in adult neutropenic patients (defined as absolute neutrophil count ≤500 cells/mm3 at baseline) with invasive candidiasis was assessed in a prospective, double-blind, randomized, controlled trial. Eligible patients received either anidulafungin (200 mg intravenous loading dose followed by 100 mg intravenous daily) or caspofungin (70 mg intravenous loading dose followed by 50 mg intravenous daily) (2:1 randomization). Patients were treated for at least 14 days. In clinically stable patients, a switch to oral azole therapy was permitted after at least 10 days of study treatment. A total of 14 neutropenic patients with microbiologically confirmed invasive candidiasis (MITT population) were enrolled in the study (11 anidulafungin; 3 caspofungin). The majority of patients had candidemia only. The most common pathogens isolated at baseline were C. tropicalis (4 anidulafungin, 0 caspofungin), C. parapsilosis (2 anidulafungin, 1 caspofungin), C. krusei (2 anidulafungin, 1 caspofungin), and C. ciferrii (2 anidulafungin, 0 caspofungin). The successful global response rate at the End of Intravenous Treatment (primary endpoint) was 8/11 (72.7%) for anidulafungin and 3/3 (100.0%) for caspofungin (difference -27.3, 95% CI -80.9, 40.3); the successful global response rate at the End of All Treatment was 8/11 (72.7%) for anidulafungin and 3/3 (100.0%) for caspofungin (difference -27.3, 95% CI -80.9, 40.3). All-cause mortality up to the 6 Week Follow-Up visit for anidulafungin (MITT population) was 4/11 (36.4%) and 2/3 (66.7%) for caspofungin.
Patients with microbiologically confirmed invasive candidiasis (MITT population) and neutropenia were identified in an analysis of pooled data from 4 similarly designed prospective, open-label, non-comparative studies. The efficacy of anidulafungin (200 mg intravenous loading dose followed by 100 mg intravenous daily) was assessed in 35 adult neutropenic patients defined as absolute neutrophil count ≤500 cells/mm3 or WBC ≤500 cells/mm3 in 22 patients or classified by the investigator as neutropenic at baseline in 13 patients. All patients were treated for at least 14 days. In clinically stable patients, a switch to oral azole therapy was permitted after at least 5 to 10 days of treatment with anidulafungin. The majority of patients had candidemia only (85.7%). The most common pathogens isolated at baseline were C. tropicalis (12 patients), C. albicans (7 patients), C. glabrata (7 patients), C. krusei (7 patients), and C. parapsilosis (6 patients). The successful global response rate at the End of Intravenous Treatment (primary endpoint) was 18/35 (51.4%) and 16/35 (45.7%) at the End of All Treatment. All-cause mortality by Day 28 was 10/35 (28.6%). The successful global response rate at End of Intravenous Treatment and End of All Treatment were both 7/13 (53.8%) in the 13 patients with neutropenia assessed by investigators at baseline.
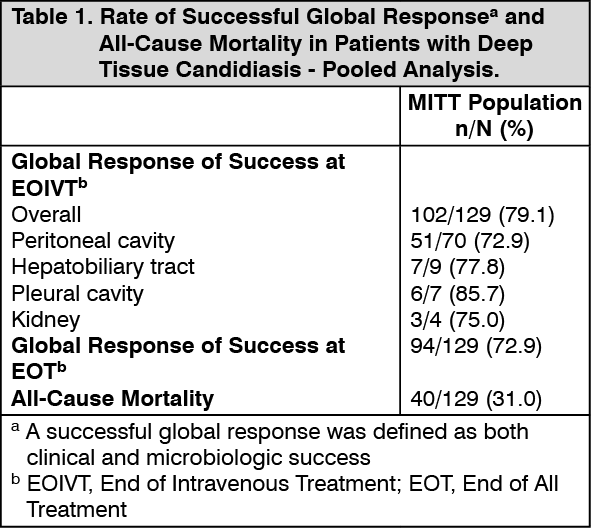
Deep Tissue Infections: The efficacy of anidulafungin (200 mg intravenous loading dose followed by 100 mg intravenous daily) in adult patients with microbiologically confirmed deep tissue candidiasis was assessed in an analysis of pooled data from 5 prospective studies (1 comparative and 4 open-label). Patients were treated for at least 14 days. In the 4 open-label studies, a switch to oral azole therapy was permitted after at least 5 to 10 days of treatment with anidulafungin. A total of 129 patients were included in the analysis. Twenty one (16.3%) had concomitant candidemia. The mean APACHE II score was 14.9 (range, 2 - 44). The most common sites of infection included the peritoneal cavity (54.3%; 70 of 129), hepatobiliary tract (7.0%; 9 of 129), pleural cavity (5.4%; 7 of 129) and kidney (3.1%; 4 of 129). The most common pathogens isolated from a deep tissue site at baseline were C. albicans (64.3%; 83 of 129), C. glabrata (31.0%; 40 of 129), C. tropicalis (11.6%; 15 of 129), and C. krusei (5.4%; 7 of 129). The successful global response rate at the end of intravenous treatment (primary endpoint) and end of all treatment and all-cause mortality up to the 6 week follow-up visit is shown in Table 1. (See Table 1.)
 Click on icon to see table/diagram/image
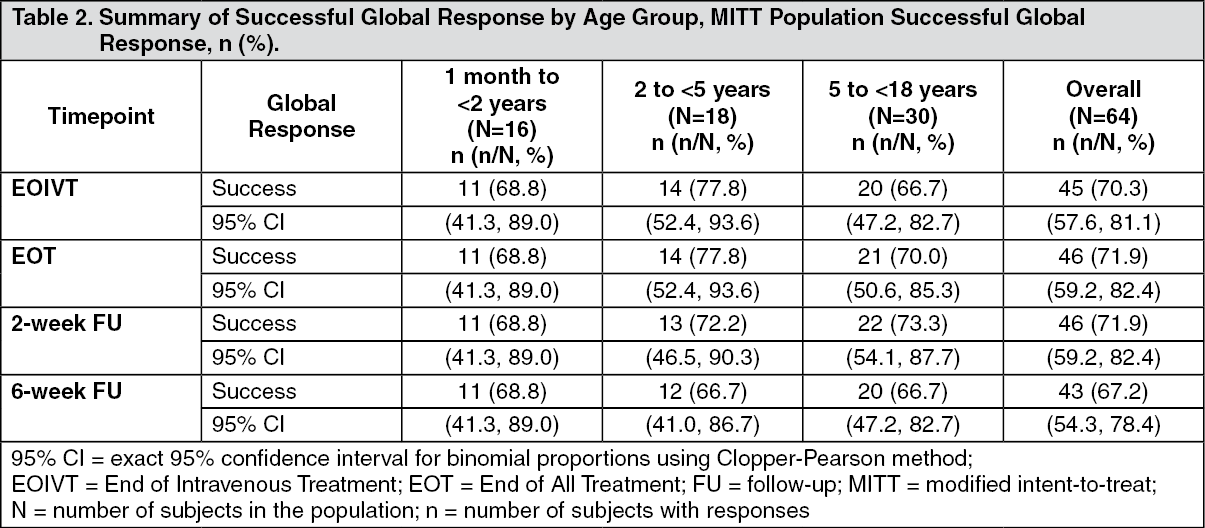
Click on icon to see table/diagram/imagePaediatric population: A prospective, open-label, non-comparative, multi-national study assessed the safety and efficacy of anidulafungin in 68 paediatric patients aged 1 month to <18 years with invasive candidiasis including candidaemia (ICC). Patients were stratified by age (1 month to <2 years, 2 to <5 years, and 5 to <18 years) and received once daily intravenous anidulafungin (3.0 mg/kg loading dose on Day 1, and 1.5 mg/kg daily maintenance dose thereafter) for up to 35 days followed by an optional switch to oral fluconazole (6-12 mg/kg/day, maximum 800 mg/day). Patients were followed at 2 and 6 weeks after EOT.
Among 68 patients who received anidulafungin, 64 had microbiologically confirmed Candida infection and were evaluated for efficacy in the modified intent-to-treat (MITT) population. Overall, 61 patients (92.2%) had Candida isolated from blood only. The most commonly isolated pathogens were Candida albicans (25 [39.1%] patients), followed by Candida parapsilosis (17 [26.6%] patients), and Candida tropicalis (9 [14.1%] patients). A successful global response was defined as having both a clinical response of success (cure or improvement) and a microbiological response of success (eradication or presumed eradication). The overall rates of successful global response in the MITT population are presented in Table 2. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePharmacokinetics: General Pharmacokinetic Characteristics: The pharmacokinetics of anidulafungin have been characterized in healthy subjects, special populations and patients. A low intersubject variability in systemic exposure (coefficient of variation of approximately 25%) was observed. The steady state was achieved on the first day after a loading dose (twice the daily maintenance dose).
Distribution: The pharmacokinetics of anidulafungin are characterized by a rapid distribution half-life (0.5-1 hour) and a volume of distribution of 30-50 L that is similar to total body fluid volume. Anidulafungin is extensively bound (>99%) to human plasma proteins.
Biotransformation: Hepatic metabolism of anidulafungin has not been observed. Anidulafungin is not a clinically relevant substrate, inducer, or inhibitor of cytochrome P450 isoenzymes. It is unlikely that anidulafungin will have clinically relevant effects on the metabolism of drugs metabolized by cytochrome P450 isoenzymes.
Anidulafungin undergoes slow chemical degradation at physiologic temperature and pH to a ring-opened peptide that lacks antifungal activity. The in vitro degradation half-life of anidulafungin under physiologic conditions is approximately 24 hours. In vivo, the ring-opened product is subsequently converted to peptidic degradants and eliminated mainly through biliary excretion.
Elimination: The clearance of anidulafungin is about 1 L/h. Anidulafungin has a predominant elimination half-life of approximately 24 hours that characterizes the majority of the plasma concentration-time profile and a terminal half-life of 40-50 hours that characterizes the terminal elimination phase of the profile.
In a single-dose clinical study, radiolabeled (14C) anidulafungin (~88 mg) was administered to healthy subjects. Approximately 30% of the administered radioactive dose was eliminated in the feces over 9 days, of which less than 10% was intact drug. Less than 1% of the administered radioactive dose was excreted in the urine. Anidulafungin concentrations fell below the lower limits of quantitation 6 days post-dose. Negligible amounts of drug-derived radioactivity were recovered in blood, urine, and feces 8 weeks post-dose.
Linearity: Anidulafungin displays linear pharmacokinetics across a wide range of once daily doses (15-130 mg).
Special Populations: Patients with Fungal Infections: The pharmacokinetics of anidulafungin in patients with fungal infections are similar to those observed in healthy subjects based on population pharmacokinetic analyses. With the 200/100 mg daily dose regimen at an infusion rate of 1 mg/min, the steady-state Cmax and trough concentrations Cmin could reach approximately 7 and 3 mg/L, respectively, with an average steady-state AUC of approximately 110 mg·h/L.
Weight: Though weight was identified as a source of variability in clearance in the population pharmacokinetic analysis, weight has little clinical relevance on the pharmacokinetics of anidulafungin.
Gender: Plasma concentrations of anidulafungin in healthy men and women were similar. In multiple-dose patient studies, drug clearance was slightly faster (approximately 22%) in men.
Elderly: The population pharmacokinetic analysis showed that median clearance differed slightly between the elderly group (patients ≥65, median CL = 1.07 L/h) and the non-elderly group (patients <65, median CL = 1.22 L/h), however, the range of clearance was similar.
Ethnicity: Anidulafungin pharmacokinetics were similar among Caucasian, Blacks, Asians, and Hispanics.
HIV Positivity: Dosage adjustments are not required based on HIV positivity, irrespective of concomitant anti-retroviral therapy.
Hepatic Insufficiency: Anidulafungin is not hepatically metabolized. Anidulafungin pharmacokinetics were examined in subjects with Child-Pugh class A, B or C hepatic insufficiency. Anidulafungin concentrations were not increased in subjects with any degree of hepatic insufficiency. Although a slight decrease in AUC was observed in patients with Child-Pugh C hepatic insufficiency, the decrease was within the range of population estimates noted for healthy subjects.
Renal Insufficiency: Anidulafungin has negligible renal clearance (<1%). In a clinical study of subjects with mild, moderate, severe or end stage (dialysis-dependent) renal insufficiency, anidulafungin pharmacokinetics were similar to those observed in subjects with normal renal function. Anidulafungin is not dialyzable and may be administered without regard to the timing of hemodialysis.
Paediatric: The pharmacokinetics of anidulafungin after daily doses were investigated in 24 immunocompromised pediatric (2 to 11 years old) and adolescent (12 to 17 years old) patients with neutropenia. The steady state was achieved on the first day after a loading dose (twice the maintenance dose), and the steady state Cmax and AUCss increase in a dose-proportional manner. The systemic exposures following the daily maintenance doses, 0.75 and 1.5 mg/kg/day in patients aged 2 to 17 years old were comparable to those observed in adults following 50 and 100 mg/day, respectively.
The pharmacokinetics of anidulafungin was investigated in 66 paediatric patients (1 month to <18 years) with ICC in a prospective, open-label, non-comparative paediatric study following administration of 3.0 mg/kg loading dose and 1.5 mg/kg/day maintenance dose (see Pharmacodynamics as previously mentioned). Based on population pharmacokinetic analysis of combined data from adult and paediatric patients with ICC, the mean exposure parameters (AUC0-24,ss and Cmin,ss) at steady state in the overall paediatric patients across age groups (1 month to <2 years, 2 to <5 years, and 5 to <18 years) were comparable to those in adults receiving 200 mg loading dose and 100 mg/day maintenance dose. Body weight adjusted CL (L/h/kg) and volume of distribution at steady state (L/kg) were similar across the age groups.
Toxicology: Preclinical safety data: Non-clinical data reveal no special hazards for humans based on conventional studies of safety pharmacology, acute toxicity, repeated dose toxicity, and toxicity to reproduction. In 3 month studies, evidence of liver toxicity, including elevated enzymes and morphologic alterations, was observed in both rats and monkeys at doses 4 to 6-fold higher than the anticipated clinical therapeutic exposure. In vitro and in vivo genotoxicity studies with anidulafungin provided no evidence of genotoxic potential. Long-term studies in animals have not been conducted to evaluate the carcinogenic potential of anidulafungin.
Administration of anidulafungin to rats did not indicate any effects on reproduction, including male and female fertility.
Anidulafungin crossed the placental barrier in rats and was detected in fetal plasma. The potential risk to the human fetus is unknown.
Anidulafungin was found in the milk of lactating rats. It is not known whether anidulafungin is excreted in human milk.
Anidulafungin did not produce any drug-related developmental toxicity in rats at the highest dose of 20 mg/kg/day, a dose equivalent to 2 times the proposed therapeutic maintenance dose of 100 mg on the basis of relative body surface area. Developmental effects observed in rabbits (slightly reduced fetal weights) occurred in the high dose group, a dose that also produced maternal toxicity.
Results of pharmacokinetic-pharmacodynamic studies in rabbit models of disseminated candidiasis and hematogenous Candida meningoencephalitis indicated that higher doses of anidulafungin were needed to optimally treat infections of CNS tissues relative to non-CNS tissues.
Studies conducted in juvenile rats did not indicate a greater susceptibility to anidulafungin hepatotoxicity compared to adult animals.