


 Sign Out
Sign Out
The incidence of adverse reactions was determined using a pre-specified pool of patients from 13 short-term (mean duration 22 weeks), placebo-controlled studies in type 2 diabetes. Across these 13 studies, 2360 patients were treated once daily with FORXIGA 10 mg and 2295 were treated with placebo (either as monotherapy or in combination with other antidiabetic therapies).
Additionally, FORXIGA 5 mg was evaluated in a 12-study, short-term, placebo-controlled pool of type 2 diabetes patients that included 1145 patients treated with FORXIGA 5 mg (mean exposure = 22 weeks) and 1393 patients treated with placebo (mean exposure = 21 weeks), either as monotherapy or in combination with other antidiabetic therapies.
In the dedicated cardiovascular (CV) outcomes study in patients with type 2 diabetes mellitus (DECLARE), 8574 patients received FORXIGA 10 mg and 8569 received placebo for a median exposure time of 48 months. In total, there were 30623 patient-years of exposure to FORXIGA.
In the dapagliflozin cardiovascular outcome study in patients with heart failure with reduced ejection fraction (DAPA-HF), 2368 patients were treated with dapagliflozin 10 mg and 2368 patients with placebo for a median exposure time of 18 months. The patient population included patients with type 2 diabetes mellitus and without diabetes, and patients with eGFR ≥30 mL/min/1.73 m2. In the dapagliflozin cardiovascular outcome study in patients with heart failure with left ventricular ejection fraction (LVEF) >40% (DELIVER), 3126 patients were treated with dapagliflozin 10 mg and 3127 patients with placebo for a median exposure time of 27 months. The patient population included patients with type 2 diabetes mellitus and without diabetes, and patients with eGFR ≥25 mL/min/1.73 m2.
In the dapagliflozin renal outcome study in patients with chronic kidney disease (DAPA-CKD), 2149 patients were treated with dapagliflozin 10 mg and 2149 patients with placebo for a median exposure of 27 months. The patient population included patients with type 2 diabetes mellitus and without diabetes, with eGFR ≥25 and ≤75 mL/min/1.73 m2. Treatment was continued if eGFR fell to levels below 25 mL/min/1.73 m2.
The safety profile of dapagliflozin was overall consistent across the studied indications. DKA was observed only in patients with diabetes mellitus.
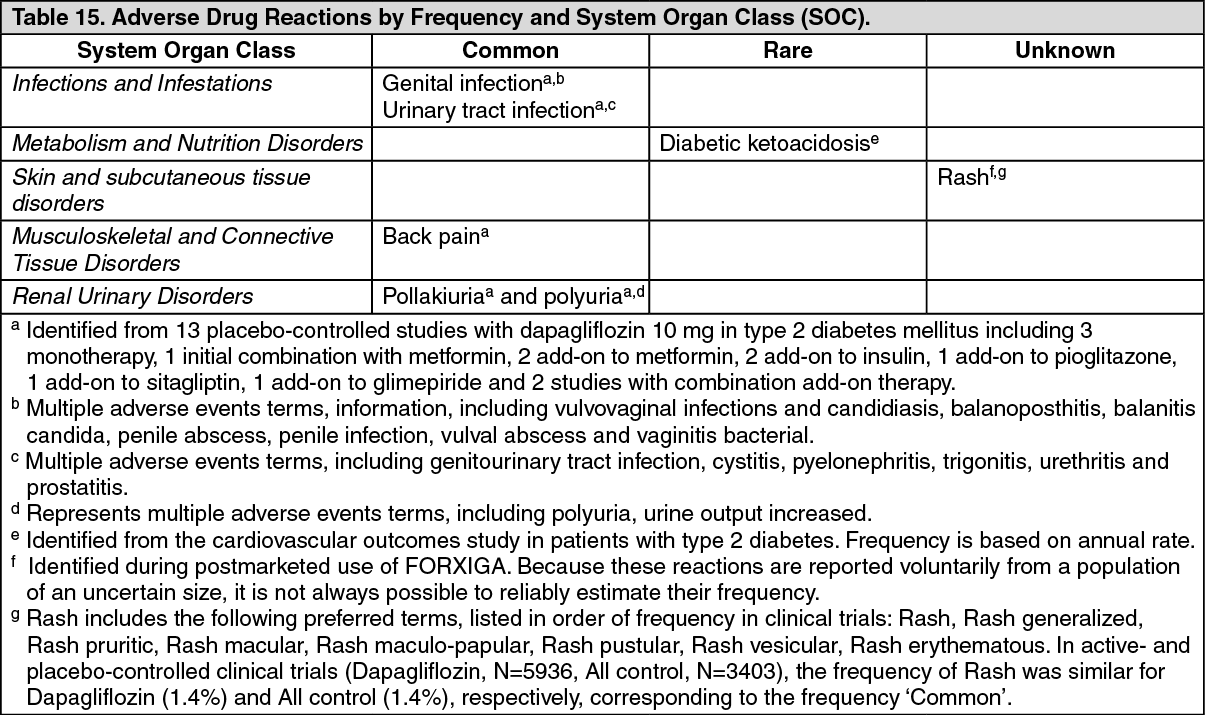
Adverse reactions: The adverse reactions in patients treated with FORXIGA 10 mg in clinical trials and postmarketing are shown in Table 15. (See Table 15.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse events observed in studies in type 2 diabetes mellitus: Genital Infections: Events of genital infections were reported in 5.5% and 0.6% of patients who received FORXIGA 10 mg and placebo, respectively, in the 13-study short-term, placebo-controlled pool. The events of genital infections reported in patients treated with FORXIGA 10 mg were all mild to moderate. Most events of genital infection responded to an initial course of standard treatment and rarely resulted in discontinuation from the study (0.2% FORXIGA 10 mg versus 0% in placebo). Infections were reported more frequently in females (8.4% FORXIGA 10 mg versus 1.2% placebo) than in males (3.4% FORXIGA 10 mg versus 0.2% placebo). The most frequently reported genital infections were vulvovaginal mycotic infections in females, and balanitis in males.
Overall, treatment with FORXIGA 5 mg was similar to treatment with FORXIGA 10 mg.
In the DECLARE study, the number of patients with serious adverse events (SAE) of genital infections were few and balanced: 2 (<0.1%) patients in each of the FORXIGA and placebo groups.
In the DAPA-HF study, no patient reported a SAE of genital infections in the FORXIGA group and one in the placebo group. There were 7 (0.3%) patients with adverse events leading to discontinuations (DAE) due to genital infections in the FORXIGA group and none in the placebo group. In the DELIVER study, one (<0.1%) patient in each treatment group reported a SAE of genital infections. There were 3 (0.1%) patients with DAEs due to genital infection in the FORXIGA group and none in the placebo group.
In the DAPA-CKD study, there were 3 (0.1%) patients with SAE of genital infections in the FORXIGA group and none in the placebo group. There were 3 (0.1%) patients with DAEs due to genital infections in the FORXIGA group and none in the placebo group.
Urinary tract infections: Events of urinary tract infections (UTI) were reported in 4.7% and 3.5% of patients who received FORXIGA 10 mg and placebo, respectively, in the 13-study short-term, placebo-controlled pool.
Most events of urinary tract infections reported in patients treated with FORXIGA 10 mg were mild to moderate. Most patients responded to an initial course of standard treatment, and urinary tract infections rarely caused discontinuation from the study (0.2% FORXIGA 10 mg versus 0.1% placebo). Infections were more frequently reported in females (8.5% FORXIGA 10 mg versus 6.7% placebo) than in males (1.8% FORXIGA 10 mg versus 1.3% placebo).
In the DECLARE study there were fewer patients with SAEs of UTI in the FORXIGA group compared with the placebo group: 79 (0.9%) and 109 (1.3%), respectively.
The number of patients with SAEs of UTI were low and balanced in the DAPA-HF and DELIVER studies: in DAPA-HF there were: 14 (0.6%) patients in the FORXIGA group and 17 (0.7%) in the placebo group and in DELIVER there were 41 (1.3%) patients in the FORXIGA group and 37 (1.2%) in the placebo group. In the DAPA-HF study, there were 5 (0.2%) patients with DAEs due to UTI in each of the FORXIGA and placebo groups. In the DELIVER study, there were 13 (0.4%) patients with DAEs due to UTI in the FORXIGA group and 9 (0.3%) in the placebo group.
In the DAPA-CKD study, there were 29 (1.3%) patients with SAEs of UTI in the FORXIGA group and 18 (0.8%) patients in the placebo group. There were 8 (0.4%) patients with DAEs due to UTI in the FORXIGA group and 3 (0.1%) in the placebo group.
Diabetic ketoacidosis (DKA): Type 2 diabetes mellitus: In the DECLARE study with a median exposure time of 48 months, events of DKA were reported in 27 patients in the FORXIGA 10 mg group and 12 patients in the placebo group. The events occurred evenly distributed over the study period. Of the 27 patients with DKA events in the FORXIGA group, 22 had concomitant insulin treatment at the time of the event. Precipitating factors for DKA were as expected in a type 2 diabetes mellitus population (see Precautions).
In the DAPA-HF study, events of DKA were reported in 3 patients with type 2 diabetes mellitus in the FORXIGA group and none in the placebo group. In the DELIVER study, events of DKA were reported in 2 patients with type 2 diabetes mellitus in the FORXIGA group and none in the placebo group.
In the DAPA-CKD study, events of DKA were not reported in any patient in the FORXIGA group and in 2 patients with type 2 diabetes mellitus in the placebo group.
View ADR Monitoring Form