


 Sign Out
Sign Out

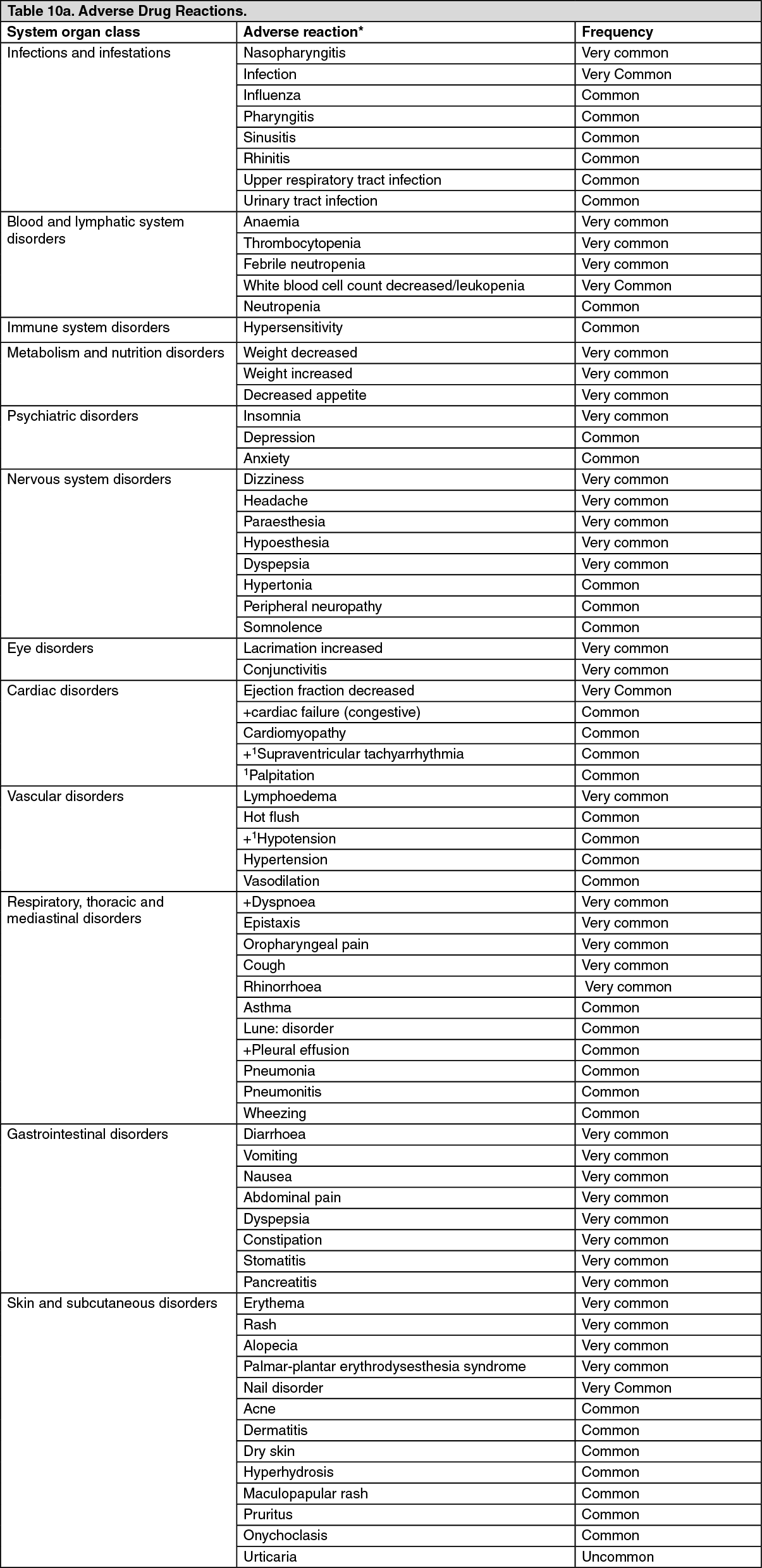
List of adverse reactions: Presented in the following table are adverse reactions that have been reported in association with the use of trastuzumab alone or in combination with chemotherapy in pivotal clinical trials. All the terms included are based on the highest percentage seen in pivotal clinical trials.
As trastuzumab is commonly used with other chemotherapeutic agents and radiotherapy it is often difficult to ascertain the causal relationship of an adverse event to a particular drug/radiotherapy. (See Table 10.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image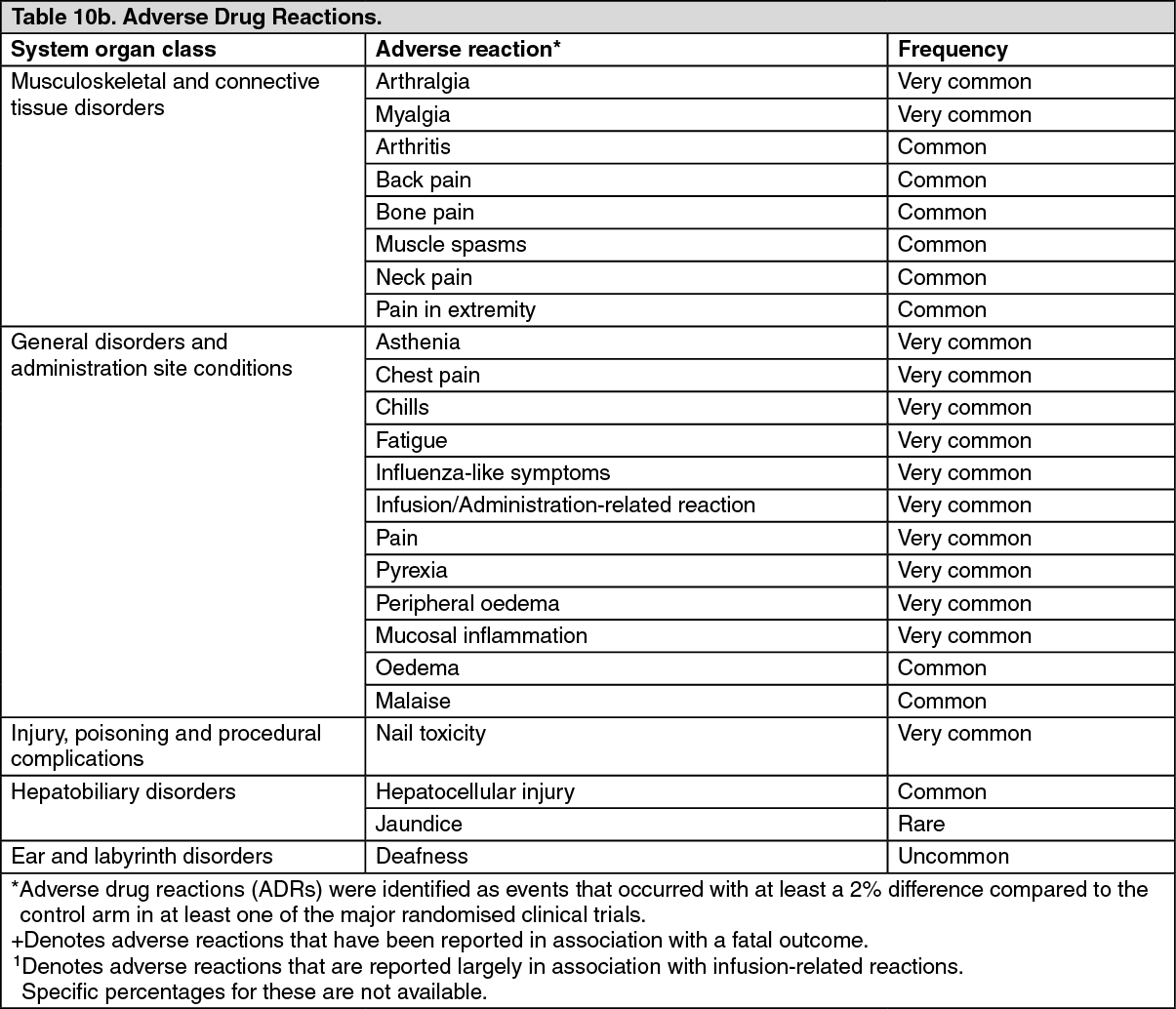 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageImmunogenicity: In the neoadjuvant-adjuvant setting, 7.1% of patients treated with the IV infusion developed antibodies against trastuzumab (regardless of antibody presence at baseline).
The clinical relevance of these antibodies is not known; however, the pharmacokinetics, efficacy [determined by pathological complete response (pCR)] or safety [determined by occurrence of administration related reactions (ARRs)] of trastuzumab IV did not appear to be adversely affected by these ADAs.
Infusion/Administration-related reactions (IRRs/ARRs) and hypersensitivity: IRRs/ARRs such as chills and/or fever, dyspnoea, hypotension, wheezing, bronchospasm, tachycardia, reduced oxygen saturation and respiratory distress were seen in all trastuzumab clinical trials and for the IV formulation (see Precautions).
IRRs/ARRs may be clinically difficult to distinguish from hypersensitivity reactions.
The rate of IRRs/ARRs of all grades varied between studies depending on the indication, whether trastuzumab was given concurrently with chemotherapy or as monotherapy and data collection methodology.
In MBC, the rate of IRRs ranged from 49% to 54% in the trastuzumab containing arm compared to 36% to 58% in the comparator arm (which may have contained other chemotherapy). Severe (grade 3 and above) ranged from 5% to 7% in the trastuzumab containing arm compared to 5 to 6% in the comparator arm.
In EBC, the rate of IRRs/ARRs ranged from 18% to 54% in the trastuzumab containing arm compared to 6% to 50% in the comparator arm (which may have contained other chemotherapy). Severe (grade 3 and above) ranged from 0.5% to 0.6% in the trastuzumab containing arm compared to 0.3 to 5% in the comparator arm.
Anaphylactoid reactions were observed in isolated cases.
Cardiac dysfunction: Congestive heart failure (NYHA II-IV) is a common adverse reaction to trastuzumab. It has been associated with fatal outcome. Signs and symptoms of cardiac dysfunction such as dyspnoea, orthopnoea, increased cough, pulmonary oedema, S gallop, or reduced ventricular ejection fraction, have been observed in patients treated with trastuzumab (see Precautions).
Metastatic Breast Cancer: Depending on the criteria used to define cardiac dysfunction, the incidence in the pivotal metastatic trials varied between 9% and 12% in the trastuzumab + paclitaxel subgroup, compared with 1% - 4% for the paclitaxel alone subgroup. For trastuzumab monotherapy, the rate was 6% - 9%. The highest rate of cardiac dysfunction was seen in patients receiving concurrent trastuzumab + anthracycline/cyclophosphamide (27%), significantly higher than in the anthracycline/cyclophosphamide alone subgroup (7% - 10%). In a subsequent trial with prospective monitoring of cardiac function, the incidence of symptomatic heart failure was 2.2% in patients receiving trastuzumab and docetaxel, compared with 0% in patients receiving docetaxel alone. Most of the patients (79%) who developed cardiac dysfunction in these trials experienced an improvement after receiving standard treatment for CHF.
Early Breast Cancer (adjuvant setting): In three pivotal clinical trials of adjuvant trastuzumab given in combination with chemotherapy the incidence of grade 3/4 cardiac dysfunction (symptomatic CHF) was similar in patients who were administered chemotherapy alone and in patients who were administered trastuzumab sequentially to a taxane (0.3 - 0.4%).
The rate was highest in patients who were administered trastuzumab concurrently with a taxane (2.0%). At 3 years, the cardiac event rate in patients receiving AC->P (doxorubicin plus cyclophosphamide followed by paclitaxel) + H (trastuzumab) was estimated at 3.2%, compared with 0.8% in AC->P treated patients. No increase in the cumulative incidence of cardiac events was seen with further follow-up at 5 years.
At 5.5 years, the rates of symptomatic cardiac or LVEF events were 1.0%, 2.3%, and 1.1% in the AC->D (doxorubicin plus cyclophosphamide, followed by docetaxel), AC->DH (doxorubicin plus cyclophosphamide, followed by docetaxel plus trastuzumab), and DCarbH (docetaxel, carboplatin and trastuzumab) treatment arms, respectively. For symptomatic CHF (Grade 3 - 4), the 5-year rates were 0.6%, 1.9%, and 0.4% in the AC->D, AC->DH, and DCarbH treatment arms, respectively. The overall risk of developing symptomatic cardiac events was low and similar for patients in AC->D and DCarbH arms; relative to both the AC->D and DCarbH arms there was an increased risk of developing a symptomatic cardiac event for patients in the AC->DH arm, being discernable by a continuous increase in the cumulative rate of symptomatic cardiac or LVEF events up to 2.3% compared to approximately 1% in the two comparator arms (AC->D and DCarbH).
When trastuzumab was administered after completion of adjuvant chemotherapy NYHA class III-IV heart failure was observed in 0.6% of patients in the one-year arm after a median follow-up of 12 months. After a median follow-up of 3.6 years the incidence of severe CHF and left ventricular dysfunction after 1 year trastuzumab therapy remained low at 0.8% and 9.8%, respectively.
In study BO16348, after a median follow-up of 8 years the incidence of severe CHF (NYHA III & IV) in the trastuzumab 1 year treatment was 0.89%, and the rate of mild symptomatic and asymptomatic left ventricular dysfunction was 6.35%.
Reversibility of severe CHF (defined as a sequence of at least two consecutive LVEF values 2: 50% after the event) was evident for 71.4% of trastuzumab-treated patients. Reversibility of mild symptomatic and asymptomatic left ventricular dysfunction was demonstrated for 79.5% of trastuzumab-treated patients. Approximately 17% of cardiac dysfunction related events occurred after completion of trastuzumab.
In the joint analysis of studies NSABP B-31 and NCCTG N9831, with a median follow-up of 8.1 years for the AC->PH group (doxorubicin plus cyclophosphamide, followed by paclitaxel plus trastuzumab), the per patient incidence of new onset cardiac dysfunction, as determined by LVEF, remained unchanged compared to the analysis performed at a median follow up of 2.0 years in the AC->PH group: 18.5% of AC->PH patients with LVEF decreased of 2:10% to below 50%. Reversibility of left ventricular dysfunction was reported in 64.5% of patients who experienced a symptomatic CHF in the AC->PH group being asymptomatic at latest follow up, and 90.3% having full or partial LVEF recovery (88).
Early Breast Cancer (neoadjuvant-adjuvant setting): In the clinical trial setting, when trastuzumab was administered concurrently with neoadjuvant chemotherapy containing three to four cycles of a neoadjuvant anthracycline (cumulative doxorubicin dose 180 mg/m2 or epirubicin dose 360 mg/m2) overall, the incidence of symptomatic cardiac dysfunction was up to 1.7% in the trastuzumab arm.
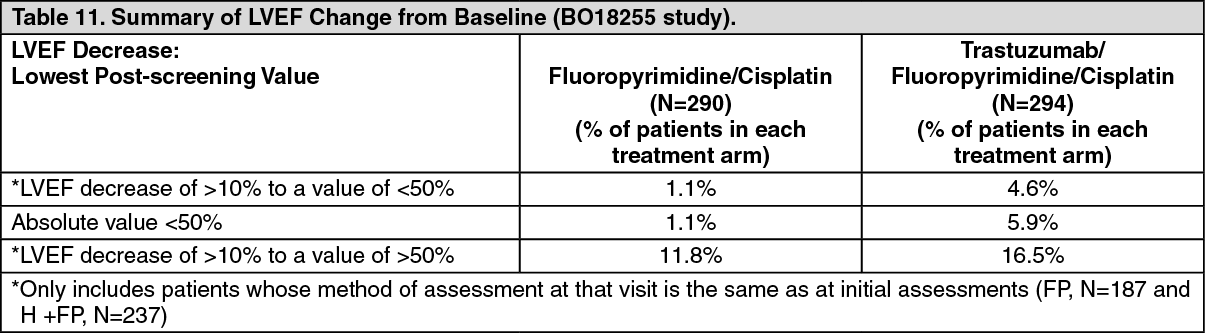
Advanced Gastric Cancer: In the BO18255 study, at screening, the median LVEF value was 64% (range 48%-90%) in the fluoropyrimidine/cisplatin arm (FP) and 65% (range 50%-86%) in the trastuzumab plus fluoropyrimidine/cisplatin arm (H+FP).
The majority of the LVEF decreases noted in BO18255 study were asymptomatic, with the exception of one patient in the trastuzumab-containing arm whose LVEF decrease coincided with cardiac failure. (See Tables 11 and 12.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image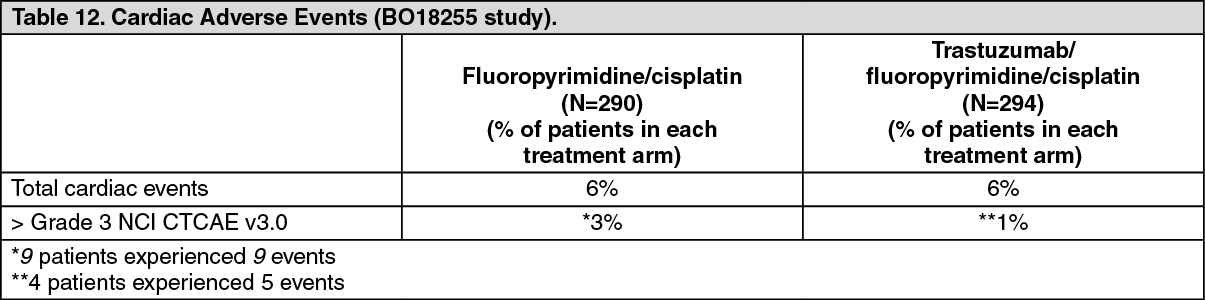 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageOverall, there were no significant differences in cardiac dysfunction between the treatment arm and the comparator arm.
Haematological toxicity: Breast Cancer: Haematological toxicity is infrequent following the administration of trastuzumab monotherapy in the metastatic setting, WHO Grade 3 leukopenia, thrombocytopenia and anaemia occurring in < 1% of patients. No WHO Grade 4 toxicities were observed. There was an increase in WHO Grade 3 or 4 haematological toxicity in patients treated with the combination of trastuzumab and paclitaxel compared with patients receiving paclitaxel alone (34% versus 21%). Haematological toxicity was also increased in patients receiving trastuzumab and docetaxel, compared with docetaxel alone (32% Grade 3/4 neutropenia versus 22%, using NCI-CTC criteria). The incidence of febrile neutropenia/neutropenic sepsis was also increased in patients treated with trastuzumab + docetaxel (23% versus 17% for patients treated with docetaxel alone).
Using NCI-CTC criteria, in the BO16348 study, 0.4% of trastuzumab-treated patients experienced a shift of 3 or 4 grades from baseline, compared with 0.6% in the observation arm.
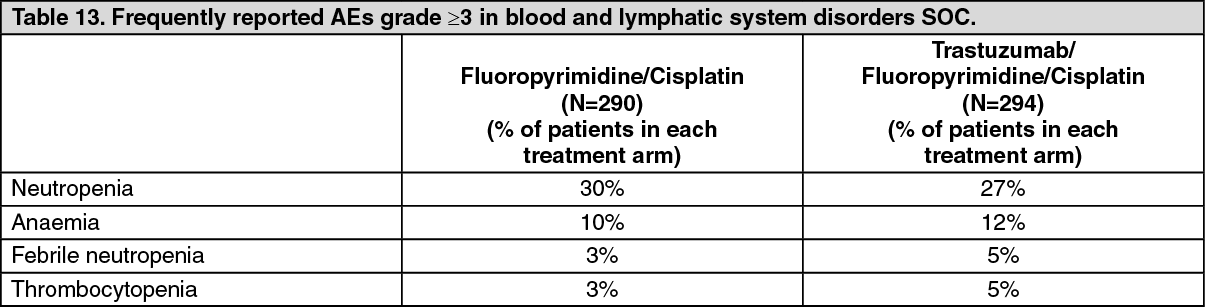
Advanced Gastric Cancer: The most frequently reported AEs, of Grade ≥3 occurring with an incidence rate of at least 1% by trial treatment, that were categorised under the Blood and Lymphatic System Disorders SOC are shown as follows: See Table 13.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe total percentage of patients who experienced an AE of ≥ Grade 3 NCI-CTCAE v3.0 that has been categorized under this SOC were 38% in the FP arm and 40% in the FP + H arm.
Overall, there were no significant differences in haematotoxicity between the treatment arm and the comparator arm.
Hepatic and renal toxicity: Breast Cancer: WHO Grade 3 or 4 hepatic toxicity was observed in 12% of patients following administration of trastuzumab as single agent, in the metastatic setting. This toxicity was associated with progression of disease in the liver in 60% of these patients.
WHO Grade 3 or 4 hepatic toxicity was less frequently observed among patients receiving trastuzumab and paclitaxel than among patients receiving paclitaxel alone (7% compared with 15%). No WHO Grade 3 or 4 renal toxicity was observed.
Advanced Gastric Cancer: In the BO18255 study no significant differences in hepatic and renal toxicity were observed between the two treatment arms.
NCI-CTCAE (version 3.0) Grade ≥ 3 renal toxicity was not significantly higher in patients receiving trastuzumab than those in the F+P arm (3% and 2% respectively).
NCI-CTCAE (version 3.0) Grade ≥ 3 adverse event in the Hepatobiliary Disorders SOC: Hyperbilirubinaemia was the only reported AE and was not significantly higher in patients receiving trastuzumab than those in the F+P arm (1% and < 1% respectively).
Diarrhoea: Breast Cancer: Of patients treated with trastuzumab monotherapy in the metastatic setting 27% experienced diarrhoea. An increase in the incidence of diarrhoea, primarily mild to moderate in severity, has also been observed in patients receiving trastuzumab in combination with paclitaxel compared with patients receiving paclitaxel alone.
In the BO16348 study, 8% of trastuzumab-treated patients experienced diarrhoea during the first year of treatment.
Advanced Gastric Cancer: In the BO18255 study, 109 patients (37%) participating in the trastuzumab-containing treatment arm versus 80 patients (28%) in the comparator arm experienced any grade diarrhoea. Using NCI-CTCAE v3.0 severity criteria, the percentage of patients experiencing Grade ≥ 3 diarrhoea was 4% in the FP arm versus 9% in the FP+H arm.
Infection: An increased incidence of infections, primarily mild upper respiratory infections of minor clinical significance or catheter infections, has been observed in patients treated with trastuzumab.
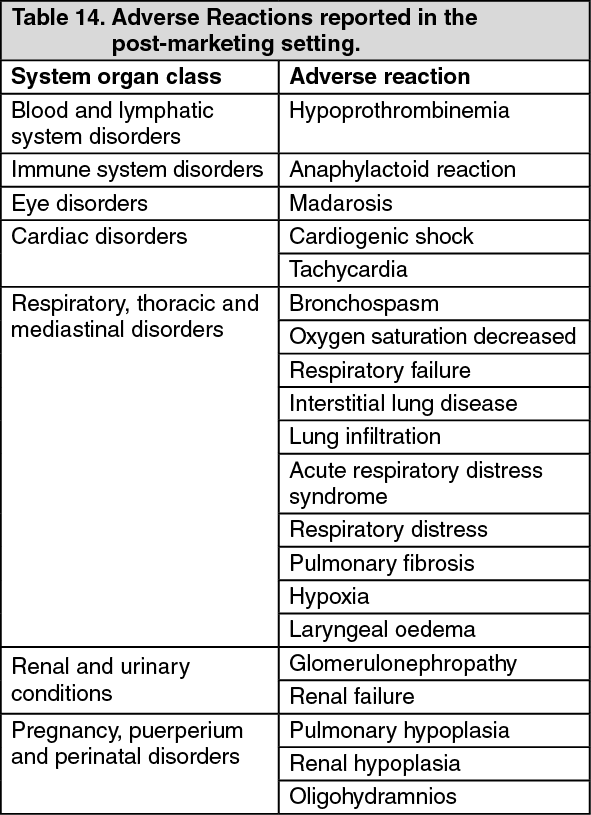
Post Marketing: See Table 14.
 Click on icon to see table/diagram/image
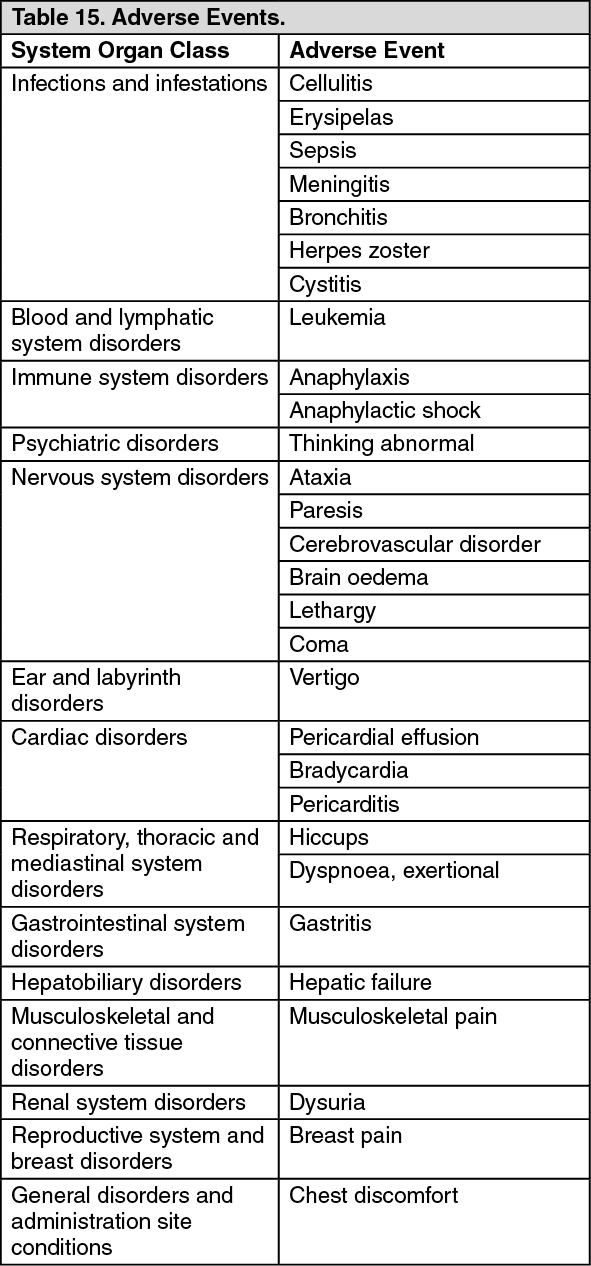
Click on icon to see table/diagram/imageAdverse Events: Table 15 as follows indicates adverse events that historically have been reported in patients who have received trastuzumab. As no evidence of a causal association has been found between trastuzumab and these events, these events are not considered expected for the purposes of regulatory reporting. (See Table 15.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
View ADR Monitoring Form