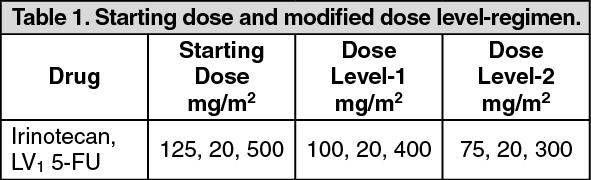
Combination Therapy: Irinotecan can be administered in two different regimens in combination with 5-fluorouracil and leucovorin for the treatment of colorectal cancer. Irinotecan 125 mg/m
2 is administered as IV on 90 min on days-1, 8, 15, and 22 followed by leucovorin 20 mg/m
2 as IV bolus on same days. 5-fluorouracil should be administered immediately after administration of leucovorin at a dose of 500 mg/m
2 thereafter the additional courses are repeated after every 6 weeks (4 weeks on therapy, 2 weeks off therapy). After initiation of chemotherapy the patient should be carefully monitored for toxicity and dose of irinotecan, LV and 5-FU should be modified as necessary to accommodate individual patient's tolerance to treatment. See Table 1.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Irinotecan 180 mg/m
2 is administered as IV over 90 minutes on days 1, 15, 29 followed by LV 200 mg/m
2 over 2 hours on days 1, 2, 15, 16, 29 and 30.
5-FU should be administered immediately after administration of LV at a dose of 400 mg/m
2 IV bolus. The bolus of 5-FU should be followed by infusional 5-FU at a dose of 600 mg/m
2 over 22 hours on days 1, 2, 15, 16, 29 and 30. Next course begins on day 43.
After initiation of chemotherapy the patient should be carefully monitored for toxicity and doses of irinotecan, LV and 5-FU should be modified as necessary to accommodate individual patient's tolerance to treatment. See Table 2.
Click on icon to see table/diagram/image
Preparation and Administration: As with other potentially toxic anticancer agents, care should be exercised in the handling and preparation of infusion solutions prepared from irinotecan injection. The use of gloves is recommended. If a solution of irinotecan contacts the skin, wash the skin immediately and thoroughly with soap and water. If irinotecan contacts the mucous membranes, flush thoroughly with water.
Preparation of Infusion Solution: Inspect vial contents for particulate matter and repeat inspection when drug product is withdrawn from vial into syringe. Irinotecan must be diluted prior to infusion. Irinotecan should be diluted in 5% Dextrose Injection, USP, (preferred) or 0.9% Sodium Chloride Injection, USP, to a final concentration range of 0.12 to 2.8 mg/mL.
The solution is physically and chemically stable for up to 24 hours at room temperature (approximately 25°C) and in ambient fluorescent lighting. Because of possible microbial contamination during dilution, it is advisable to use the admixture prepared with 5% Dextrose Injection, USP, within 24 hours if refrigerated (2° to 8°C, 36° to 46°F). In the case of admixtures prepared with 5% Dextrose Injection, USP, or Sodium Chloride Injection, USP, the solutions should be used within 6 hours if kept at room temperature (15°C to 30°C, 59° to 86°F). Other drugs should not be added to the infusion solution.
Refrigeration of admixtures using 0.9% Sodium Chloride Injection is not recommended because of an incidence of visible particulates. Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration whenever solution and container permit.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image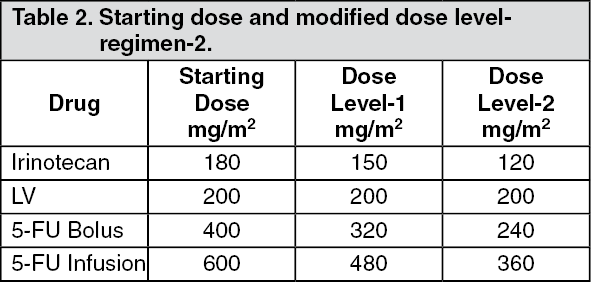 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out