


 Sign Out
Sign Out

Pharmacology: Pharmacodynamics: Lantus is an antidiabetic agent, which contains insulin glargine. Insulin glargine is a human insulin analogue designed to have a low solubility at neutral pH. At pH 4, insulin glargine injection solution is completely soluble.
After injection into the subcutaneous tissue, the acidic solution is neutralised, leading to the formation of micro-precipitates from which small amounts of insulin glargine are released continuously, yielding a smooth, peakless, predictable concentration/time profile with a prolonged duration of action.
Insulin glargine is metabolised into 2 active metabolites M1 and M2 (see Pharmacokinetics: Metabolism as follows).
Insulin receptor binding: In vitro studies indicate that the affinity of insulin glargine and its metabolites M1 and M2 for the human insulin receptor is similar to the one of human insulin.
IGF-1 receptor binding: The affinity of insulin glargine for the human IGF-1 receptor is approximately 5 to 8-fold greater than that of human insulin (but approximately 70 to 80-fold lower than the one of IGF-1), whereas M1 and M2 bind the IGF-1 receptor with slightly lower affinity compared to human insulin.
The total therapeutic insulin concentration (insulin glargine and its metabolites) found in type 1 diabetic patients was markedly lower than what would be required for a half-maximal occupation of the IGF-1 receptor and the subsequent activation of the mitogenic-proliferative pathway initiated by the IGF-1 receptor. Physiological concentrations of endogenous IGF-1 may activate the mitogenic-proliferative pathway; however, the therapeutic concentrations found in insulin therapy, including in Lantus therapy, are considerably lower than the pharmacological concentrations required to activate the IGF-1 pathway.
In euglycaemic clamp studies in healthy subjects or in patients with type 1 diabetes, the onset of action of subcutaneous insulin glargine was slower than with human NPH insulin, its effect profile was smooth and peakless, and the duration of its effect was prolonged. To illustrate this, the following graph shows the activity profiles over time of insulin glargine and NPH insulin in patients with type 1 diabetes: See figure.
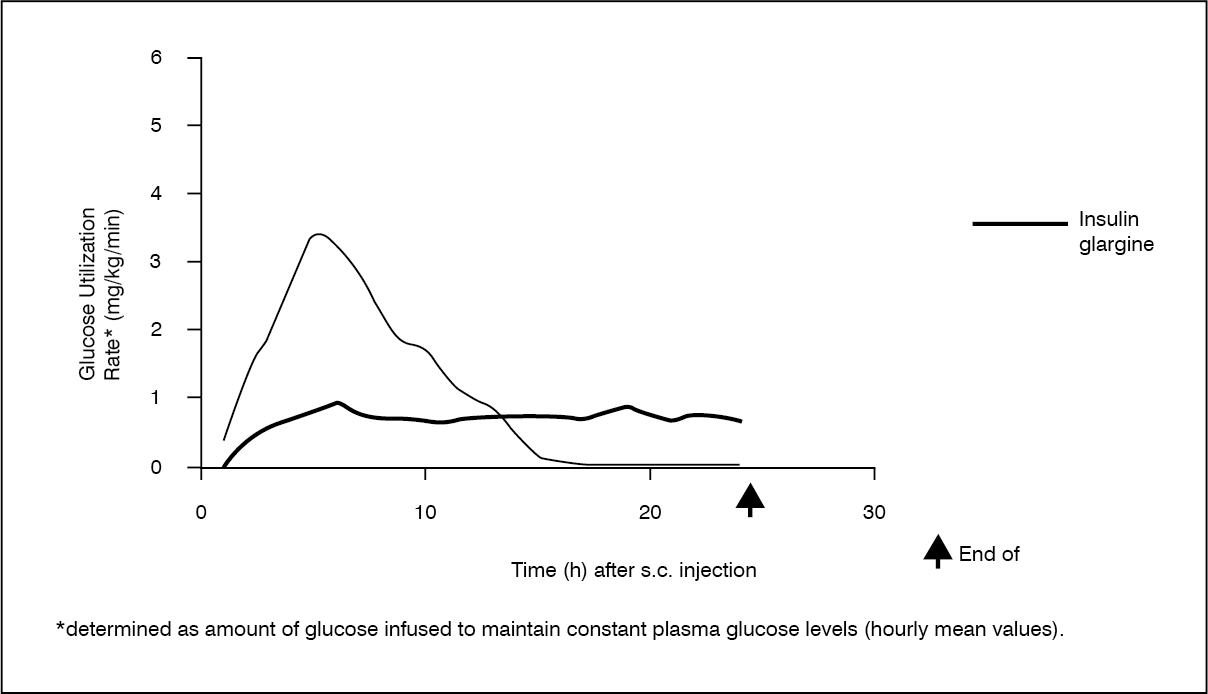 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe longer duration of action of insulin glargine is directly related to its slower rate of absorption and supports once daily administration. The time course of action of insulin and insulin analogues such as insulin glargine may vary considerably in different individuals or within the same individual.
There were no clinically relevant differences in serum insulin levels after abdominal, deltoid or thigh administration of insulin glargine.
Clinical Efficacy: Type 1 Paediatric diabetes (1 to 6 years): A 24-week parallel group study was conducted in 125 children with type 1 diabetes mellitus 1 to 6 years (61 children from 2 to 5 in the insulin glargine group and 64 children from 1 to 6 in the NPH insulin group), comparing insulin glargine given once daily in the morning to NPH insulin given once or twice daily as basal insulin. Both groups received bolus insulin before meals.
Comparison of the 2 treatment regimens in terms of hypoglycemia was the primary objective of the study. The composite primary outcome consisted of continuous glucose monitoring excursions below 70 mg/dL (3.9 mM), confirmed by fingerstick blood glucose (FSBG) measurements; other FSBG measurements < 70 mg/dL; and episodes of symptomatic hypoglycemia. Overall, the event rate ratio of this composite outcome for once daily Lantus compared to NPH (given twice daily in most patients) was 1.18 (95% CI: 0.97-1.44), therefore, not meeting the non-inferiority margin of 1.15.
The rate of symptomatic hypoglycemia events is the most commonly used and clinically relevant component of the composite outcome. Rates of symptomatic hypoglycemia events were numerically lower in the insulin glargine group, both overall (25.5 episodes per patient-year, vs 33.0 for NPH) and overnight (2.38 episodes per patient-year, vs 3.65 for NPH).
Glycohaemoglobin and glucose variabilities were comparable in both treatment groups. No new safety signals were observed in this trial.
ORIGIN Trial (Study 4032): The ORIGIN (Outcome Reduction with Initial Glargine INtervention) trial was a, international, multicenter, randomized, 2x2 factorial design study conducted in 12,537 participants with impaired fasting glucose (IFG), impaired glucose tolerance (IGT) or early type 2 diabetes mellitus and evidence of CV disease. Participants were randomized to receive Lantus (n=6264), titrated to a FPG of 95 mg/dL (5.3mM) or less, or Standard Care (n=6273). At baseline participants had a mean age of 63.5 years, mean duration of diabetes of 5.8 years in those with pre-existing diabetes, and median HbA1c of 6.4%. Median duration of follow-up was approximately 6.2 years.
At the end of the trial 81% of participants randomized to take Lantus were still on treatment. Median on-treatment HbA1c values ranged from 5.9 to 6.4% in the Lantus group, and 6.2% to 6.6% in the Standard Care group throughout the duration of follow-up. Median FPG in the Lantus group was at target (≤ 95mg/dL) following dose titration for the duration of the study.
The rates of severe hypoglycemia (affected participants per 100 participant years of exposure) were 1.05 for insulin glargine and 0.30 for Standard Care group. Overall, severe hypoglycemia was reported for 3.7% of these participants over the course of this 6 year study (approximately 0.6% per participant-year). The median of the change in body weight from baseline to the last on-treatment visit was 2.2 kg greater in the Lantus group than in the Standard Care group.
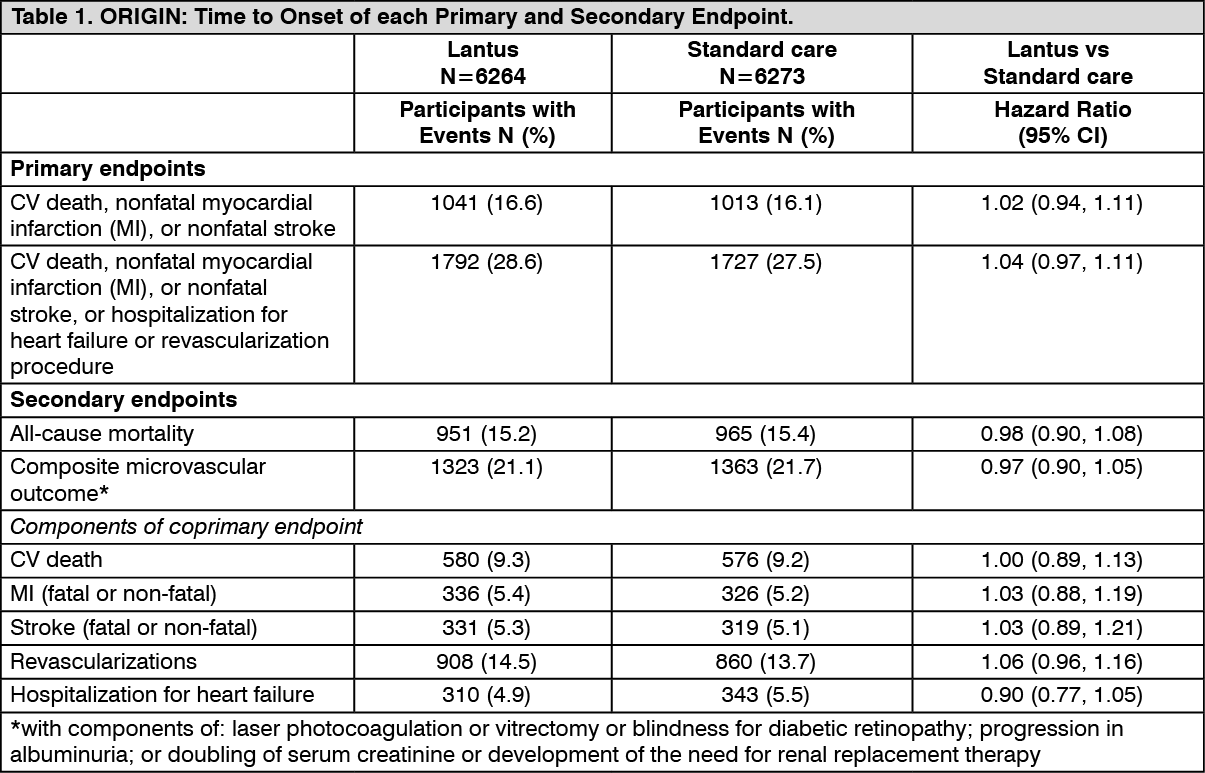
The primary objective of this trial was to examine the effect of Lantus on two co-primary composite efficacy outcomes. The first one was the time to the first occurrence of CV death, nonfatal myocardial infarction (MI), or nonfatal stroke, and the second one was the time to the first occurrence of any of the first co-primary events, or revascularization procedure (cardiac, carotid, or peripheral), or hospitalization for heart failure.
Secondary endpoints were: all-cause mortality; a composite microvascular outcome; development of type 2 diabetes, in participants with IGT and/or IFG at baseline.
The primary and secondary outcome results, as well as the results for each component of the coprimary outcomes, are displayed in the two tables (Table 1 for the time-to-event analyses, and, for the non-time-to event analysis of development of diabetes, Table 2) as follows. (See Tables 1 and 2).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image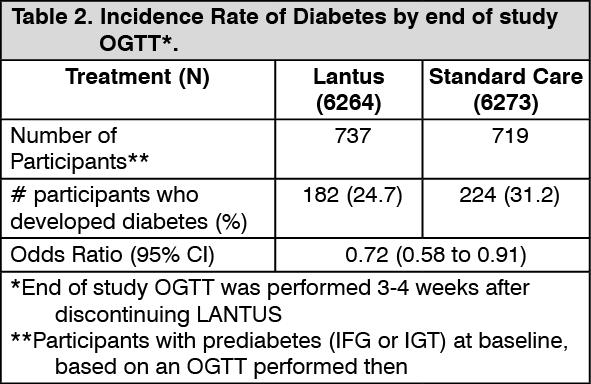 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThere were no statistical significant differences between treatment groups in the overall incidence of cancer (all types combined) or death from cancer. The time to first event of any cancer or new cancer during the study was similar between the two treatment groups with respective hazard ratios of 0.99 (0.88, 1.11) and 0.96 (0.85, 1.09).
Participation in ORIGIN for a median of approximately 6.2 years showed that treatment with Lantus did not alter the risk for cardiovascular outcomes, all-cause mortality or cancer, when compared to standard glucose lowering therapy. In addition, metabolic control was maintained at a lower level of glycemia, with a decrease in the percentage of participants developing diabetes, at a cost of a modest increase in hypoglycemia and weight gain.
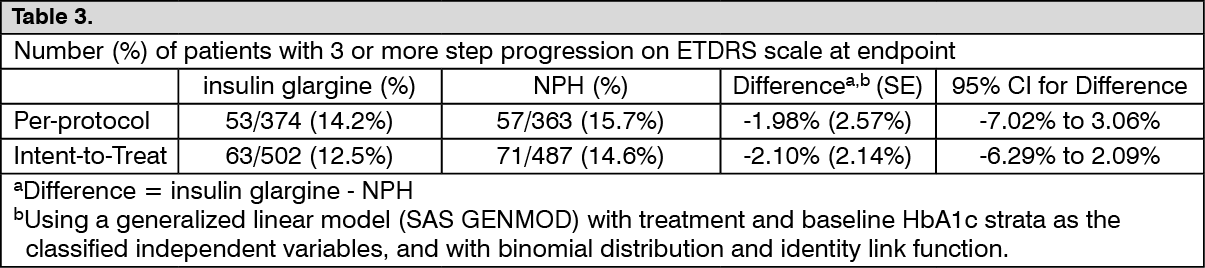
Diabetic Retinopathy: Effects of insulin glargine on diabetic retinopathy were evaluated in a large 5-year NPH-controlled study in which progression of retinopathy was investigated by fundus photography using a grading protocol derived from the Early Treatment Diabetic Retinopathy Study (ETDRS). The primary outcome in this study was progression by 3 or more steps on the ETDRS scale at study endpoint. The results of this analysis are shown in the table as follows for both the per-protocol (primary) and Intent-to-Treat (ITT) populations, and indicate noninferiority of insulin glargine to NPH in the progression of diabetic retinopathy as assessed by this outcome. (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePharmacokinetics: Distribution: After subcutaneous injection of insulin glargine in healthy subjects and diabetic patients, the insulin serum concentrations indicated a slower and much more prolonged absorption and a lack of a peak in comparison to human NPH insulin. Concentrations were, thus, consistent with the time profile of the pharmacodynamic activity of insulin glargine.
After subcutaneous injection of 0.3 U/kg insulin glargine in diabetic patients, a concentration-time profile without pronounced peak as compared to NPH-insulin has been observed.
When given intravenously, the concentration profiles and the apparent elimination half-life of insulin glargine and human insulin were comparable.
Metabolism: After SC injection of Lantus in healthy subjects and diabetic patients, insulin glargine is rapidly metabolized at the carboxyl terminus of the Beta chain with formation of two active metabolites M1 (21A-Gly-insulin) and M2 (21A-Gly-des-30B-Thr-insulin). In plasma, the principal circulating compound is the metabolite M1. The exposure to M1 increases with the administered dose of Lantus. The pharmacokinetic and pharmacodynamic findings indicate that the effect of the subcutaneous injection with Lantus is principally based on exposure to M1. Insulin glargine and the metabolite M2 were not detectable in the vast majority of subjects and, when they were detectable their concentration was independent of the administered dose of Lantus.
Special Populations: Children: Pharmacokinetics in children aged 2 to less than 6 years with type 1 diabetes mellitus was assessed in one clinical study (see Pharmacodynamics as previously mentioned). Plasma "trough" levels of insulin glargine and its main metabolites M1 and M2 were measured in children treated with insulin glargine, revealing plasma concentration patterns similar to adults, and providing no evidence for accumulation of insulin glargine or its metabolites with chronic dosing.