


 Sign Out
Sign Out
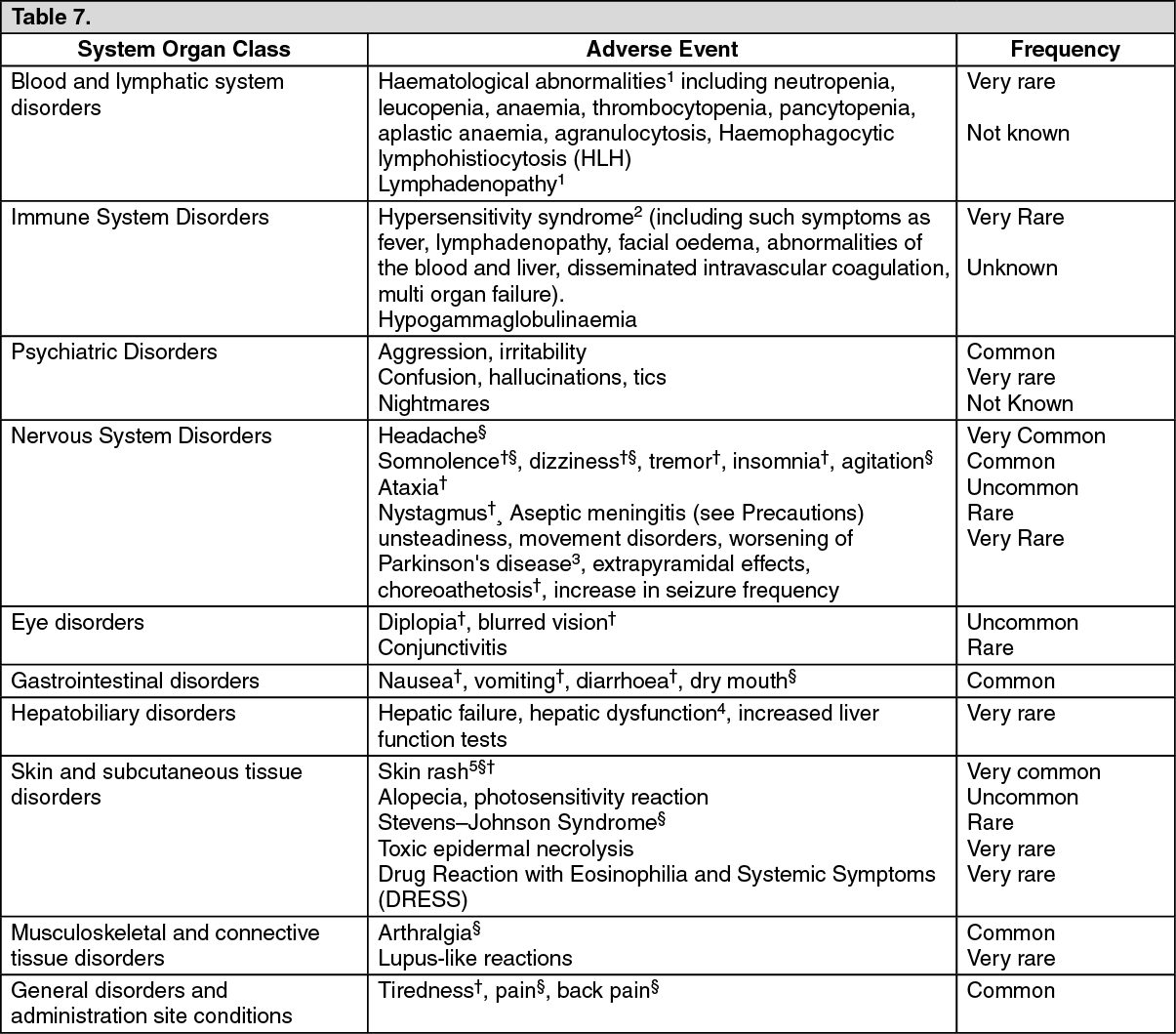
The following convention has been utilised for the classification of undesirable effects: Very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1000 to <1/100); rare (≥1/10,000 to <1/1000); very rare (<1/10,000), not known (cannot be estimated from the available data). (See Table 7.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: 1Haematological abnormalities and lymphadenopathy may or may not be associated with the hypersensitivity syndrome (see Immune System Disorders as previously mentioned in Table 7).
2Rash has also been reported as part of a hypersensitivity syndrome associated with a variable pattern of systemic symptoms including fever, lymphadenopathy, facial oedema and abnormalities of the blood and liver. The syndrome shows a wide spectrum of clinical severity and may, rarely, lead to disseminated intravascular coagulation and multiorgan failure. It is important to note that early manifestations of hypersensitivity (for example fever, lymphadenopathy) may be present even though rash is not evident. If such signs and symptoms are present, the patient should be evaluated immediately and lamotrigine tablets discontinued if an alternative aetiology cannot be established.
3These effects have been reported during other clinical experience.
There have been reports that lamotrigine may worsen parkinsonian symptoms in patients with pre-existing Parkinson's disease, and isolated reports of extrapyramidal effects and choreoathetosis in patients without this underlying condition.
4Hepatic dysfunction usually occurs in association with hypersensitivity reactions but isolated cases have been reported without overt signs of hypersensitivity.
5In clinical trials in adults, skin rashes occurred in up to 8-12% of patients taking lamotrigine and in 5-6% of patients taking placebo. The skin rashes led to the withdrawal of lamotrigine treatment in 2% of patients. The rash, usually maculopapular in appearance, generally appears within eight weeks of starting treatment and resolves on withdrawal of lamotrigine tablets (see Precautions).
Serious potentially life-threatening skin rashes, including Stevens-Johnson syndrome and toxic epidermal necrolysis (Lyell's Syndrome) have been reported. Although the majority recover on withdrawal of lamotrigine treatment, some patients experience irreversible scarring and there have been rare cases of associated death (see Precautions).
The overall risk of rash, appears to be strongly associated with: high initial doses of lamotrigine and exceeding the recommended dose escalation of lamotrigine therapy (see Dosage & Administration); concomitant use of valproate (see Dosage & Administration).
Rash has also been reported as part of a hypersensitivity syndrome associated with a variable pattern of systemic symptoms (see Immune System Disorders as previously mentioned in Table 7).
There have been reports of decreased bone mineral density, osteopenia, osteoporosis and fractures in patients on long-term therapy with lamotrigine. The mechanism by which lamotrigine affects bone metabolism has not been identified.
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product.
Healthcare professionals are asked to report any suspected adverse reactions via Yellow Card Scheme.
Website: www.mhra.gov.uk/yellowcard.
View ADR Monitoring Form