The information highlighted (if any) are the most recent updates for this brand.
The target INR range of oral anticoagulant therapy: Prophylaxis of thromboembolic complications in patients with prosthetic heart valves: INR 2.5-3.5. Other indications: INR 2.0-3.0.
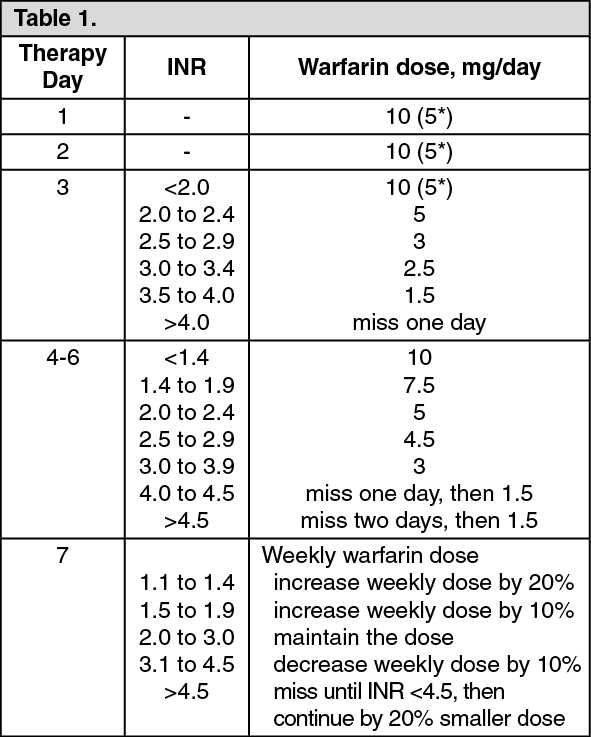
Adults: Patients in normal weight and the spontaneous INR under 1.2 are administered 10 mg of warfarin on three consecutive days. The dosing is continued according to the table as follows based on the INR measured on the fourth day.
In open care and for patients with inherited protein C or protein S deficiency the recommended initial dose is 5 mg of warfarin (*) in three days. The dosing is continued according to the table as follows, based on the INR-measured on the fourth day. (See Table 1.)
For elderly patients, for those small in size, for those with the spontaneous INR over 1.2, or for those who have a disease (see Precautions) or medication (see Interactions) affecting the efficacy of anticoagulant therapy, the recommended initial dose is 5 mg of warfarin (*) for two days. The dosing is continued according to table 2, based on the INR measurement performed on the third day. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
INR measurements are carried out daily until the therapeutic level has been achieved (usually this takes 5 to 6 days). Intervals of INR measurements are then extended weekly. In long-term follow-up the measurement intervals are dependent i.a. on the patient's compliance and clinical status, targeting, however, on 4-weekly measurement intervals. If large fluctuations exist in the INR values or if the patient has a disease affecting liver function or the absorption of vitamin K, the measuring interval must be shorter than this. Many medicines may potentiate or weaken the effect of warfarin, which must be considered in the follow-up when initiating or discontinuing other medications. In long-term follow-up the adjustments required based on the INR measurements are made to the weekly dose. Thereafter the effect of the adjustment is checked by measuring the INR after 1 or 2 weeks of the adjustment. After this, the intervals are targeted on the same 4-weekly measurement intervals.
Children: The initiation and follow up of anticoagulant therapy in children is carried out by pediatricians. Dosage can be adjusted according to Table 2. (See Table 2.)
Click on icon to see table/diagram/image
Elective Surgery: Pre-, peri- and postoperative anticoagulant therapy the following dosage can be applied (if an urgent reversal of oral anticoagulant effect is needed, see Overdose).
Determine the INR one week prior to the scheduled surgery. Discontinue warfarin 1 to 5 days prior to surgery. If the patient is in high risk of thromboembolism, subcutaneous low molecular weight heparin should be given at therapeutic doses. The effect of heparin can be monitored by measuring the prophylactic effect of FXa when the effective therapeutic level is 0.3 to 0.7 anti-FXa activity units/mL.
The extent of warfarin pause depends on the INR value. Discontinue warfarin: 5 days prior to surgery if the INR > 4.0; 3 days prior to surgery if the INR=3.0 to 4.0; 2 days prior to surgery if the INR=2.0 to 3.0.
Determine the INR in the evening before surgery. If INR >1.8, administer 0.5 to 1 mg vitamin K
1 intravenously or orally.
Consider the need for unfractionated heparin infusion or prophylactic low molecular weight heparin during the day of surgery.
Continue subcutaneous low molecular weight heparin for 5 to 7 days concomitantly with reintroduced warfarin therapy.
Initiate warfarin with maintenance doses in the evening after minor surgery, and on the day the patient begins enteral nutrition after major surgery.
Warfarin iteracts with many drugs. Drugs may reduce the absorption or enterohepatic circulation of warfarin (cholestyramine). Drugs may induce (antiepileptics or antituberculotics) or inhibit the hepatic metabolism of warfarin (e.g, amiodarone or metronidazole). In certain instances cessation of inhibition or induction of liver enzymes can also change the balance of warfarin therapy. Certain drugs may displace warfarin from the plasma protein bonds, which increases the free fraction and, unless the patient has some liver disease or some other medication inhibiting warfarin metabolism, this generally enhances the elimination of warfarin. The best known pharmacodynamic interactions are associated with the simultaneous use of drugs affecting the platelets (acetylsalicylic acid, clopidogrel, ticlopidine, dipyridamole, most of the non-steroidal anit-inflammatory drugs, but not the coxibs). Primary and secondary hemostasis predisposes the patient to severe bleeding complications. Penicillins in large doses may have the same effect. Vitamin K-dependent synthesis of the coagulation factor is reduced and the warfarin effect is potentiated by certain drugs, such as anabolic steroids, azapropazone, erythromycin, and some cephalosporins. An ample supply of dietary vitamin K reduces the warfarin effect. Correspondingly, reduced absorption of vitamin K due to e.g. diarrhoea may potentiate the warfarin effect. In patients with inadequate supply of vitamin K, antibiotics may reduce the ability of the intestinal bacteria to produce vitamin K2, which leads to an enhanced warfarin effect. Heavy use of alcohol with concomitant hepatic failure potentiates the warfarin effect. The quinine contained in Tonic-water may also potentiate the warfarin effect.
Cranberry juice and other cranberry products may potentiate the effect of warfarin and therefore concomitant use should be avoided. If the patient needs relief of pain while on warfarin, paracetamol or opiates are recommended.
Warfarin may potentiate the effect of oral sulphonyluera antibiotics.
The following drugs have been reported to potentiate or reduce the warfarin effect: Increased Effect: Acetylsalicylic acid, allopurinol, amiodarone, amoxicillin, argatroban, azapropazone, azithromycin, bezafibrate, capecitabine, carboxyuridine, celecoxib, clarithromycin, chloral hydrate, cefamandole, cefalexin, cefmenoxime, cefmetazole, cefoperazone, cefuroxime, cimetidine, ciprofloxacin, clofibrate, codeine, cyclophosphamide, dexstropropoxphene, (dextro) thyroxine, digoxin, disulfiram, doxycycline, erythromycin, etoposide, fenofibrate, feprazone, fluconazole, fluorouracil, flutamide, flutamide, fluvastatin, fluvoxamine, gatifloxacin, gemfibrozil, grepafloxacin, ifosfamide, indometacin, influenza vaccine, interferon alpha and beta, isoniazid, itraconazole, ketoconazole, latamoxef, leflunomide, lepirudin, levofloxacin, lovastatin, metolazone, methotrexate, metronidazole, miconazole (also oral gel), moxifloxacin, nalidixic acid, norfloxacin, ofloxacin, omeprazole, oxyphenbutazone, paracetamol (the effect evident after 1 to 2 weeks of continuous use), phenylbutazone, piroxicam, proguanil, propafenone, propranolol, quinine, quinidine, rofecoxib, roxithromycin, simvastatin, sulfafurazole, sulfamethizole, sulfamethoxazole-trimethoprim, sulfaphenazole, sulfinpyrazone, sulfofenur, sulindac, (anabolic and androgenic) steroid hormones, tamoxifen, tegafur, tetracycline, tolmetin, tramadol, trastuzumab, troglitazone, valproic acid, vitamin A, vitamin E, zafirlukast.
There are reports suggesting that noscapine as wellas glucosamine with or without chondroitin sulphate may increase the INR patients on warfarin.
Decreased Effect: Azathioprine, (barbiturates), carbamazepine, chlordiazepoxide, chlortalidone, cloxacillin, ciclosporin, dicloxacillin, disopyramide, griseofulvin, mercaptopurine, mesalazine, mitotaine, nafcillin, nevirapine, phenobarbital, primidone, rifampicin, spironolactone, trazodone, vitamin C.
Herbal medication can either potentiate the warfarin effect e.g. ginkgo (Ginkgo biloba), garlic (Allium sativum), dong quai (Angelica sinensis, contains coumarins), papaya (Carica papaya) or danshen (Salvia miltiorrhiza, decreases the warfarin elemination), or reduce it, e.g. ginseng (Panax spp). The effect of warfarin can be reduced by concomitant use of the herbal preparation of St. John's wort (Hypericum perforatum). This is due to induction of drug metabolizing enzymes by St. John's wort. Herbal preparation containing St. John's wort should therefore not be combined with warfarin.
The inducing effect may persist for as long as 2 weeks after cessation of treatment with St John's wort. If a patient is already taking St John's wort check the INR and stop St John's wort. Monitor INR closely as this may rise on stopping St John's wort. The dose of warfarin may need adjusting. Ingestion of vitamin K containing foodstuffs during warfarin treatment should be as steady as possible. The most abundant vitamin K sources are green vegetables and leaves, such as: Amaranth leaf, avocado, broccoli, Brussels sprout, cabbage, canola oil, chayote leaf,chives, coriander, cucumber skin (but not cucumber without skin), endives, kale leaf, kiwifruit, lettuce leaf, mint leaf, mustard greens, olive oil, parsley, peas, pistachio nuts, purple seaweed laver, spinach leaf, spring onion, soybeans, soybean oil, tea leaves (but not tea), turnip greens, or watercress.
Topical preparations containing methyl salicylate should be used with care in patients on warfarin and excessive usage is to be avoided as potentially dangerous drug interaction can occur.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image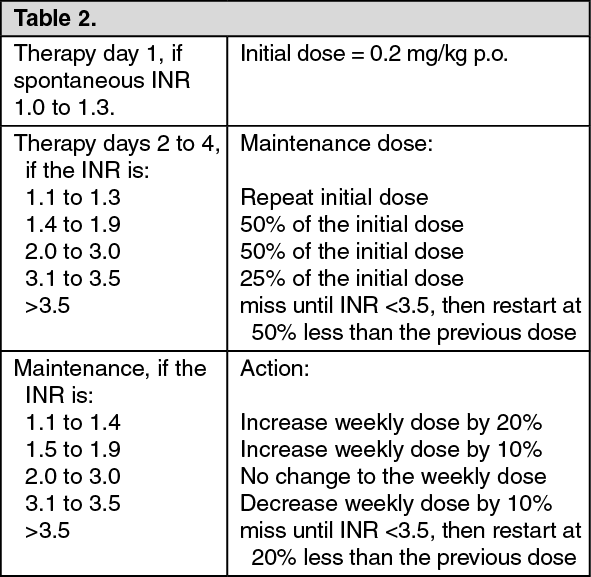 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image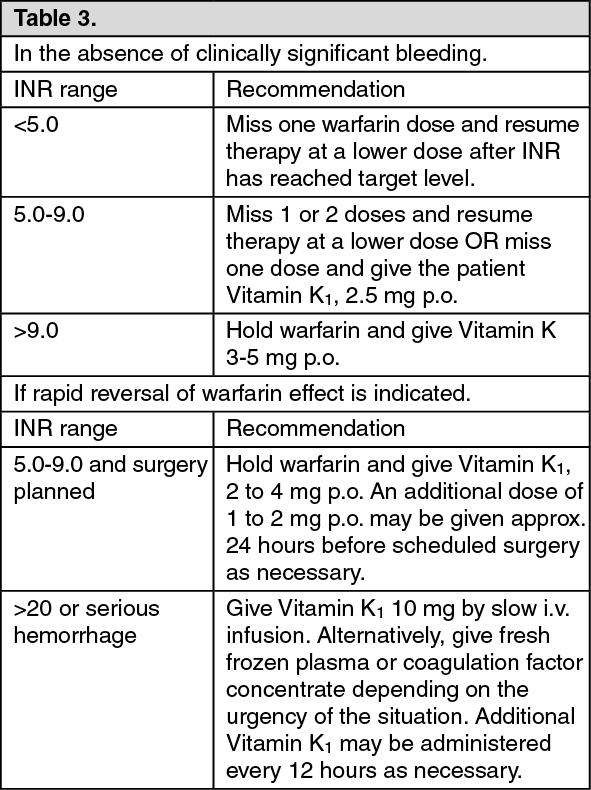 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out
