Pharmacotherapeutic group: Calcium homeostasis, anti-parathyroid agents.
ATC Code: H05BX04.
Pharmacology: Pharmacodynamics: Mechanism of Action: The calcium-sensing receptor on the surface of the chief cell of the parathyroid gland is the principal regulator of PTH secretion. Etelcalcetide is a synthetic peptide calcimimetic agent which reduces PTH secretion through binding and activation of the calcium-sensing receptor. The reduction in PTH is associated with a concomitant decrease in serum calcium and phosphate levels.
Pharmacodynamic Effects: Following a single intravenous bolus administration of 5 mg etelcalcetide, PTH levels decreased rapidly within 30 minutes post-dose and were maximally decreased for 1 hour, before returning to baseline. The extent and duration of the reduction in PTH increased with increasing dose. Reduction in PTH levels correlated with plasma etelcalcetide concentrations in haemodialysis patients. The effect of reducing PTH levels was maintained throughout the 6-month dosing period when etelcalcetide was administered by intravenous bolus 3 times a week.
Clinical efficacy and safety: Placebo-controlled studies: Two 6-month, double-blind, placebo-controlled clinical studies were conducted in SHPT patients with CKD receiving haemodialysis 3 times per week (n = 1,023). Patients were administered Parsabiv or placebo at a starting dose of 5 mg 3 times per week at the end of haemodialysis and titrated every 4 weeks through week 17 to a maximum dose of 15 mg 3 times per week to achieve target PTH level ≤ 300 pg/mL. The median average weekly dose of Parsabiv during the efficacy assessment period (EAP) was 20.4 mg (6.8 mg per administration). Patients with lower screening PTH levels typically required lower doses (median average weekly doses of 15.0 mg, 21.4 mg, 27.1 mg, respectively, for patients with screening PTH levels < 600 pg/mL, 600 to ≤ 1,000 pg/mL, and > 1,000 pg/mL). Patients were maintained on dialysate calcium concentration ≥ 2.25 meq/L.
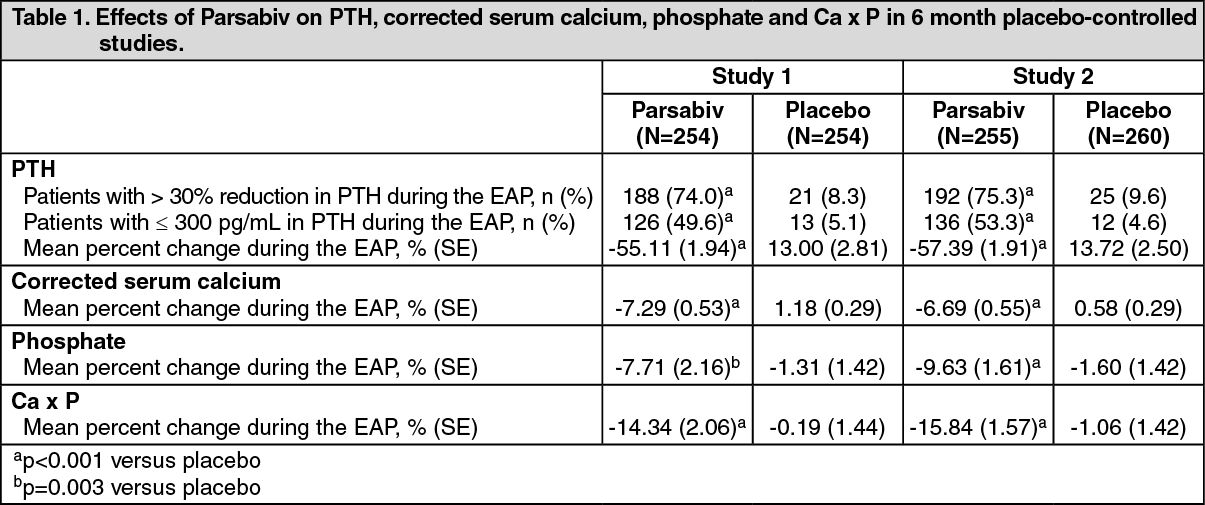
The primary endpoint in each study was the proportion of patients with > 30% reduction from baseline in PTH during the EAP (EAP, defined as weeks 20 to 27 inclusive). The secondary endpoints were the proportion of patients with a mean PTH ≤ 300 pg/mL during the EAP, and percent change from baseline during the EAP for PTH, serum cCa, phosphate and calcium phosphate product (Ca x P).
Demographic and baseline characteristics between the two groups in each study were similar. The mean age of patients across the 2 studies was 58.2 (range 21 to 93) years. Mean (SE) baseline PTH concentrations across the 2 studies were 846.9 (21.8) pg/mL, and 835.9 (21.0) pg/mL for the Parsabiv and placebo groups, respectively with approximately 21% of subjects enrolling across both studies having baseline PTH > 1,000 pg/mL. The average duration of haemodialysis prior to study entry was 5.4 years and 68% of patients were receiving vitamin D sterols at study entry, with 83% receiving phosphate binders.
Both studies demonstrated that Parsabiv reduced PTH, while lowering calcium, phosphate and Ca x P. Results of all primary and secondary endpoints were statistically significant and the results were consistent across both studies as shown in Table 1. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Parsabiv decreased PTH regardless of baseline PTH, duration of dialysis, and whether or not patients were receiving vitamin D sterols. Patients with lower screening PTH levels were more likely to reach PTH ≤ 300 pg/mL during EAP.
Parsabiv was associated with reductions in bone metabolism markers (bone specific alkaline phosphatase and type I collagen c-telopeptide) and fibroblast growth factor 23 (exploratory endpoints) at the end of the study (week 27), compared with placebo.
Active-controlled study: A 6-month, double-blind, active-controlled study compared the efficacy and safety of Parsabiv with cinacalcet in 683 SHPT patients with CKD on haemodialysis. The dosing regimen for Parsabiv was similar to that in the placebo-controlled studies (starting dose of 5 mg titrated every 4 weeks with 2.5 mg to 5 mg increments to a maximum of 15 mg 3 times a week). The starting dose of cinacalcet was 30 mg daily, titrated every 4 weeks in 30 mg increments or 60 mg for the last uptitration to a maximum dose of 180 mg daily following the cinacalcet prescribing information. The median average weekly dose of Parsabiv during the EAP was 15.0 mg (5.0 mg per administration) and of cinacalcet was 360.0 mg (51.4 mg per administration). The primary endpoint was non-inferiority for the proportion of patients who achieved > 30% reduction from baseline in mean PTH during the EAP (weeks 20 to 27). Key secondary endpoints were the proportion of patients who achieved > 50% and > 30% reductions from baseline in mean PTH during the EAP and the mean number of days of vomiting or nausea per week in the first 8 weeks, sequentially tested for superiority. Mean (SE) baseline PTH concentrations were 1,092.12 (33.8) and 1,138.71 (38.2) pg/mL for the Parsabiv and cinacalcet groups respectively. Demographics and other baseline characteristics were similar to the placebo-controlled studies.
Parsabiv was non-inferior to cinacalcet for the primary endpoint, and was superior to cinacalcet for the secondary endpoints of proportion of patients achieving > 30% reduction from baseline in mean PTH during the EAP (68.2% Parsabiv versus 57.7% cinacalcet; p = 0.004); and proportion of patients achieving >50% reduction from baseline in mean PTH during the EAP (52.4% Parsabiv versus 40.2% cinacalcet; p = 0.001). No statistically significant difference between the two groups was observed for the secondary endpoint evaluating the mean number of days of vomiting or nausea per week in the first 8 weeks.
"Switch study": Results from a study which evaluated changes in corrected serum calcium levels when switching patients from cinacalcet to Parsabiv showed that treatment with Parsabiv, at a starting dose of 5 mg, could be safely initiated after a 7-day discontinuation of cinacalcet, provided that the corrected serum calcium was ≥ 8.3 mg/dL (2.08 mmol/L).
Open-label extension study: A 52-week, single arm extension study to the placebo-controlled and "switch" studies described above was conducted to characterise the long term safety and efficacy of Parsabiv in 891 SHPT patients with CKD on haemodialysis. All subjects received Parsabiv at a starting dose of 5 mg 3 times a week. The dose of Parsabiv could be titrated at weeks 5, 9, 17, 25, 33, 41, and 49 to a maximum dose of 15 mg to achieve target PTH levels ≤ 300 pg/mL while maintaining serum cCa concentrations.
At the end of 52 weeks, Parsabiv was not associated with any new safety findings and demonstrated maintenance of treatment effect as evidenced by a decrease in pre-dialysis PTH by > 30% from baseline in 2/3rd of patients. In addition, Parsabiv decreased pre-dialysis PTH to ≤ 300 pg/mL in more than 50% of patients and decreased mean PTH, cCa, cCa x P, and phosphate from baseline.
Paediatric population: The safety and efficacy of etelcalcetide in children and adolescents less than 18 years has not yet been established. No data are available.
Pharmacokinetics: Distribution: In the population pharmacokinetics model, volume of distribution at steady-state was approximately 796 L. Etelcalcetide is predominately bound to plasma albumin by reversible covalent binding. Non-covalent binding of etelcalcetide to plasma proteins is low with a fraction unbound ratio of 0.53. The ratio of blood-to-plasma [
14C]-etelcalcetide concentrations is approximately 0.6.
Biotransformation: Etelcalcetide is not metabolised by CYP450 enzymes. Etelcalcetide is biotransformed in blood by reversible disulphide exchange with endogenous thiols to predominantly form conjugate with serum albumin. The plasma exposure of biotransformation products was approximately 5-fold higher than that of etelcalcetide and their concentration-time course parallels that of etelcalcetide. The predominant biotransformation product (albumin bound) was minimally active
in vitro.
Elimination: Intravenous administration 3 times per week at the end of a haemodialysis session resulted in an effective half-life of 3 to 5 days. Etelcalcetide is rapidly cleared in subjects with normal renal function, whilst in CKD patients requiring haemodialysis, etelcalcetide was predominantly eliminated by haemodialysis. Etelcalcetide was efficiently removed with a haemodialysis clearance value of 7.66 L/hour. Following a single radiolabelled dose of etelcalcetide in CKD patients with secondary HPT receiving haemodialysis, approximately 60% of dosed [
14C]-etelcalcetide was recovered in dialysate and approximately 7% recovered in urine and faeces combined over 175 days of collection period. The inter-subject variability of the system clearance in the patient population is approximately 70%.
Linearity/non-linearity: The pharmacokinetics of etelcalcetide is linear and does not change over time following single (5 to 60 mg) and multiple intravenous doses (2.5 to 20 mg) in CKD patients with secondary HPT receiving haemodialysis. Following 3 times a week intravenous dosing at the end of each 3 to 4 hour haemodialysis session in CKD patients, etelcalcetide plasma levels reached near steady-state 4 weeks after dosing with an observed accumulation ratio of 2- to 3-fold.
Renal impairment: No specific pharmacokinetic studies of etelcalcetide have been conducted in patients with mild to severe kidney impairment. The pharmacokinetics of etelcalcetide was characterised in CKD patients receiving haemodialysis. Etelcalcetide is intended for CKD patients receiving haemodialysis.
Hepatic impairment: No specific study in patients with hepatic impairment was performed.
Body weight, gender, age, race: No body weight, gender, age, or race-related pharmacokinetic differences have been observed in adult patients studied.
Toxicology: Preclinical safety data: The expected pharmacological effect of decreased PTH and calcium in blood were observed in animal studies at clinical exposure levels. Reductions in serum calcium associated with tremoring, convulsions and stress-related findings were observed at clinical exposure levels. All effects were reversible upon cessation of treatment.
Etelcalcetide was mutagenic in some strains of bacteria (Ames), however was not genotoxic in
in vitro and
in vivo mammalian genotoxicity assays and therefore is considered non-genotoxic in humans. In mouse and rat carcinogenicity studies, there were no etelcalcetide-related tumours up to exposure of 0.4-fold clinical exposure levels.
There was no effect on male or female fertility when etelcalcetide was administered to rats at exposure levels up to 1.8-fold higher than clinical exposures levels achieved in patients receiving etelcalcetide at 15 mg three times per week.
There were no effects on embryo-foetal development in rats and rabbits when exposed to up to 1.8 to 4.3 times clinical exposure levels during organogenesis. In a pre- and post-natal development study in rats there was a minimal increase in perinatal pup mortality, delay in parturition and transient reductions in post-natal growth associated with maternal toxicities of hypocalcaemia, tremoring, and reductions in body weight and food consumption at 1.8 times clinical exposure levels.
Studies in rats showed [
14C]-etelcalcetide was excreted in the milk at concentrations similar to plasma.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
